X



|
STUDENT DIGITAL NEWSLETTER ALAGAPPA INSTITUTIONS |

|
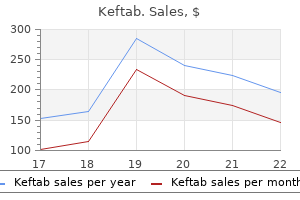
Kim M. Kerr, MD, FCCP
Her illness was readilytreatable antibiotics for neonatal uti buy keftab 250mg with visa,herinjurieswerepreventablewith afireguard antibiotics for bad uti order 125mg keftab,delayedtreatmentresultedincomplica tions and only basic medical care was available at theclinic antibiotic mic purchase keftab 750mg amex. It recognised that an integrated manage ment approach to childhood illness is required antibiotics depression cheap 250mg keftab with visa, including nutrition and preventative care in families and communities antibiotics for cystic acne treatment discount 250mg keftab. Where these are deficient infection wisdom teeth keftab 750mg lowest price, whether in developed or developing countries, children suffer, but in developing countries they not infrequently lead to death. Good doctors will continue to be admired for their ability to distil the important information from the history, for their clinical skills, for their attitude towards patients and for their knowledge of diseases, disorders and behaviour problems. They will quickly recognise doctors who demonstrate interest, empathy and concern. The continued observation of the child during the whole interview may provide important clues to the diagnosis and management. There will be occasions when the parents will not want the child present or when the child should be seen alone. The age when a child first walks is highly relevant when taking the history of a toddler but irrelevant for a teenager with headaches. Avoid having desks or beds between you and the family, but keep a comfortable distance. While the comprehensive assessment listed here is sometimes required, usually a selective approach is more appropriate (Fig. This is not an excuse for a short, slipshod history, but instead allows one to focus on the areas where a thorough, detailed history is required. Immunisations (ideally from the personal child health record) Past illnesses, hospital admissions and operations, accidents and injuries. Comprehensive history-taking is best reserved for training or for complex, multi-system disorders. If there is a positive family history, extend family pedigree over several generations. Normal growth Pubertal development (if appropriate) Feeding/drinking/appetite Any recent change in behaviour or personality. Development Check: Make sure that you and the parent or child mean the same thing when describing a problem. When first examining a young child, start at a non-threatening area, such as a hand or knee. As the examination is essential, not optional, it is best not to ask his permission, as it may well be refused! The area to be examined must be inspected fully but this is best done in stages, re-dressing the child when each stage has been completed. Developmentalskills A good overview of developmental skills can be obtained by watching the child play. A few simple toys, such as some bricks, a car, doll, ball, pencil and paper, pegboard, miniature toys and a picture book, are all that is required, as they can be adapted for any age. Inspection will provide information on: Rate of respiration is age-dependent (Table 2. Trachea: checking that it is central is seldom helpful and is disliked by children. Reduced but hyperinflated Use of accessory muscles Chest wall retraction Hyperresonant Wheeze Sputum is rarely produced by children, as they swallow it. For example, a child will not be able to jump on the spot if they have localised guarding. Kidneys these are not usually palpable beyond the neonatal period unless enlarged or the abdominal muscles are hypotonic. Corticospinal tract lesions give a dynamic pattern of movement involving shoulder adduction, forearm pronation, elbow and wrist flexion with burying of the thumb, whereas internal hip rotation and flexion at the hip and knee and plantar flexion at the ankle give a characteristic circumduction pattern of lower limb movement. If subtle, these are more evident with asking the child to adopt an unusual pattern of walking. Extrapyramidal lesions give fluctuating tone, with difficulty in initiating or involuntary movements. Duchenne muscular dystrophy) or low tone, which could be due to a central (brain) cause. Lung hyperexpansion in bronchiolitis or asthma may displace the liver and spleen downwards, mimicking hepato/splenomegaly Neurology/neurodevelopment Brief neurological screen A quick neurological and developmental overview should be performed in all children. Most children are neurologically intact and do not require formal neurological examination of reflexes, tone, etc. Specific neurological concerns or problems in development or behaviour require detailed assessment. In extra-pyramidal tract disorders, the trunk and head tend to arch backwards (extensor posturing). In muscle disease and some central brain disorders, the trunk may be hypotonic (Fig. From the age of 4 years, power can be tested formally against gravity and resistance, first testing proximal muscle and then distal muscle power and comparing sides. Absent reflexes may be due to a neuromuscular problem or a lesion within the spinal cord, but may also be due to inexpert examination technique. In spinal and cauda equina lesions there may be a palpable bladder or absent perineal sensation. If an abnormality is found, a more detailed regional examination of the affected joint as well as the joint above and below should be performed (Fig. Charts relating blood pressure to height are available and preferable; however, for convenience, charts relating blood pressure to age are often used. An abnormally high reading must be repeated, with the child relaxed, on at least three separate occasions. Passively move the joint, noting range of any restriction of movement (compare sides but note bilateral changes) Lateral and rotational movements may be as important as flexion and extension. Throat Try quickly to get a look at the tonsils, uvula, pharynx and posterior palate. In older children with headaches, diabetes mellitus or hypertension, optic fundi should be examined. Remember child protection when taking a history or examining a child where there are unusual findings. This could be reassurance, a period of observation, performing investigations or therapeutic intervention. Pattern of child development Cognitive development 31 31 32 33 34 34 Analysing developmental progress Developmental screening and assessment Child health surveillance Hearing Vision 34 41 42 42 44 3 Children acquire functional skills throughout child hood. During school age, evidence of developmentalprogressionispredominantlythrough cognitivedevelopmentandabstractthinking,although thereisalsosomefurthermaturationofearlydevelop mentalskills. Asfinemotorskillsrequire good vision, these are grouped together; similarly, normal speech and language development depends onreasonablehearingandsothesearealsoconsidered together. Of those not achieving the limit age, many will be normal late walkers, but a proportion will have an underlyingproblem,suchascerebralpalsy,aprimary muscledisorderorglobaldevelopmentaldelay. While most achieve mobility by crawling(83%),somebottomshuffleandotherscrawl withtheirabdomenonthefloor,socalledcommando crawling(creeping)(Fig. The locomotor pattern (crawling, creeping, shuffling, just standing up) determines the age of sitting,standingandwalking. Childrenwhobottomshuffleor commando crawl tend to walk later than crawlers, so thatwithinthosenotwalkingat18monthstherewill be some children who demonstrate a locomotor variantpattern,withtheirdevelopmentalprogressstill Is development normal? Normaldevelop mentimpliessteadyprogressinallfourdevelopmental fields with acquisition of skills occurring before limit agesarereached. Thisisthefundamentalconceptof learning how to think about developmental assess ment of children. Theseitemsallowthechildtorelaxbyhaving fun at the same time as facilitating observer assess mentofhisskills. Developmental screening and assessment Developmental screening(checksofwholepopulations of children at set ages by trained professionals) is a formalprocesswithinthechildhealthsurveillanceand promotionprogramme. Screening tests include the Schedule of GrowingSkillsandtheDenverDevelopmentalScreen ing Test. Those in the progressive programme include infants or children with health or developmental problems, childrenatincreasedriskofobesityorfamiliesconsid eredtobeathigherrisk,e. Many newborn infants can fix and follow horizon tallyafaceorcolouredballortheimageofatargetof concentric black and white circles. Localisation of the stimuli is not necessary and insert earphones may be usedtoobtainearspecificinformation,thusmakingit moreusefulthanfreefieldtestssuchasdistractionand performancetesting(Fig. Performance and speech discrimination testing Performance testing using high and low frequency stimuli and speech discrimination testing usingminiaturetoyscanbeusedforchildrenwithsus pected hearing loss at 18 months to 4 years of age (Fig. Developmental progress Theseveritycanbecategorisedas: mild moderate severe profound. Slow development Abnormal motor development Thismaypresentasdelayinacquisitionofmotorskills. Late walking (>18 months old) may be caused by any of the above but also needs to be differentiated fromchildrenwhodisplaythenormallocomotorvari ants of bottomshuffling or commando crawling (see Ch. Globaldevelopmentaldelay is likely to be associated with cognitive difficulties, although these may only become apparent several years later. Spastic cerebral palsy In this type, there is damage to the upper motor neurone (pyramidal or corticospinal tract) pathway. Limb tone is persistently increased (spasticity) with associated brisk deep tendon reflexes and extensor plantar responses. Dyskinetic cerebral palsy Dyskinesiareferstomovementswhichareinvoluntary, uncontrolled, occasionally stereotyped, and often moreevidentwithactivemovementorstress. In the past the commonest cause was hyperbilirubinaemia (kernicterus) due to rhesus disease of the newborn but it is now hypoxic ischaemicencephalopathyatterm. Speech and language problems are usually first sus pectedbyparentsorprimaryhealthcareprofessionals. Involvement of a neurodevelopmental paediatrician and paediatric audiological physician is indicated. Specialschooling(usuallylanguage units attached to a mainstream primary school) are available but only appropriate for a very few. Abnormal speech and language development Achildmayhaveadeficitineitherreceptiveorexpres sivespeechandlanguage,orboth. Aspergersyndromereferstoachildwiththesocial impairments of an autistic spectrum disorder but at themilderend,andnearnormalspeechdevelopment.
Executive Committee of the North American Spine Society bacteria estomacal cheap 375mg keftab fast delivery, Position statement on discography treatment for esbl uti keftab 500 mg generic, Spine antibiotics used for bronchitis order 750 mg keftab with amex, 13 (1988) 1343 antibiotic resistance laboratory purchase 750 mg keftab. Clinical Features Lumbar spinal pain infection 7 months after hysterectomy purchase 125 mg keftab with amex, with or without referred pain in the lower limb girdle or lower limb; aggravated by movements that stress the symptomatic disk antibiotics gas dogs generic keftab 250 mg line. Pathology the pathology of internal disk disruption is believed to be due to enzymatic degradation of the internal disk matrix. Initially, the degradation is restricted to the nucleus pulposus, but eventually it progresses in a centrifugal pattern along radial fissures into the anulus fibrosus. Biochemically the process involves activation of enzymes such as proteinases, cathepsin, and collagenase. Biophysically the process is characterized by denaturation and deaggregation of proteoglycans and diminished water-binding capacity of the nucleus pulposus. The causes of disk degradation are still speculative but possibly involve disinhibition of proteolytic enzymes systems endogenous to the disk as a result of impaired nutrition to the disk or injuries to the vertebral endplate. If analgesic diskography is not performed or is possibly falsenegative, criterion (3) must be explicitly satisfied. Page 181 Pain arises as a result of chemical or mechanical stimulation of the nerve endings located in the outer third or outer half of the anulus fibrosus, and is aggravated by any movements that stress these portions of the anulus. Local anesthetic blockade of the nerves supplying a target zygapophysial joint may be used as a screening procedure to determine in the first instance whether a particular joint might be the source of symptoms, but the definitive diagnosis may be made only upon selective, intraarticular injection of the putatively symptomatic joint. May be due to osteoarthrosis, but the radiographic presence of osteoarthritis is not a sufficient criterion for the diagnosis to be declared. Sprains and other injuries to the capsule of zygapophysial joints have been demonstrated at post mortem and may be the cause of pain in some patients, but these types of injuries cannot be demonstrated in vivo using currently available imaging techniques. The condition can be diagnosed only by the use of diagnostic, intraarticular zygapophysial joint blocks. For the diagnosis to be declared, all of the following criteria must be satisfied. The response must be validated by an appropriate control test that excludes falsepositive responses on the part of the patient, such as: 533. Clinical Features Lumbar spinal pain, with or without referred pain, associated with tenderness in the affected muscle and aggravated by either passive stretching or resisted contraction of that muscle. Pathology Rupture of muscle fibers, usually near their myotendinous junction, that elicits and inflammatory repair response. Remarks this nosological entity has been included in recognition of its frequent use in clinical practice, and because "muscle sprain" is readily diagnosed in injuries of the limbs. Clinical Features Lumbar spinal pain, with or without referred pain, associated with a trigger point in one or more muscles of the lumbar vertebral column. Trigger points are believed to represent areas of contracted muscle that have failed to relax as a result of failure of calcium ions to sequestrate. Page 183 Remarks For the diagnosis to be accorded, the diagnostic criteria for a trigger point must be fulfilled. Simple tenderness in a muscle without a palpable band does not satisfy the criteria, whereupon an alternative diagnosis must be accorded, such as muscle sprain, if the criteria for that condition are fulfilled, or spinal pain of unknown origin. Clinical Features Lumbar spinal pain for which there is no other underlying cause, associated with demonstrable sustained muscle activity. Diagnostic Features Palpable spasm is usually found at some time, most often in the paravertebral muscles. Remarks While there are beliefs in a pain-muscle spasm-pain cycle, clinical tests or conventional electromyography have not been shown to demonstrate reliably the presence of sustained muscle activity in such situations. Clinical Features Lumbar spinal pain, with or without referred pain, that can be aggravated by selectively stressing a particular spinal segment. Presumably involves excessive strain imposed by activities of daily living on structures such as the ligaments, joints, or intervertebral disk of the affected segment. For this diagnosis to be sustained it is critical that the clinical tests used be shown to be able to stress selectively the segment in question and to have acceptable interobserver reliability. To date, no studies have established validity for any techniques purported to demonstrate segmental dysfunction. Presumably partial rupture of the collagen fibers of the ligament at a microscopic or macroscopic level causes inflammation of the injured part. May involve sustained strain of the ligament at the limit of its physiological range at a length short of partial failure but sufficient to elicit nociceptive stimulation consistent with impending damage to the ligament. Remarks Any clinical tests or local anesthetic infiltration of the ligament must be shown to be specific for that ligament. Any conventional or otherwise established clinical tests must have been shown to have good interobserver reliability. Ligament sprain is an acceptable diagnosis in the context of injuries of the joints of the appendicular skeleton because the affected ligament is usually accessible to palpation for tenderness and because the ligament can be selectively stressed by passive movements of the related limb segments. Clinical Features Lumbar spinal pain, with or without referred pain, aggravated by active or passive movements that strain the affected ligament. Diagnostic Criteria All the following criteria should be satisfied; otherwise the diagnosis can only be presumptive. A history of an acute or chronic mechanical disturbance of the vertebral column which would be expected to have strained the specified ligament. Clinical Features Lumbar spinal pain, with or without referred pain, aggravated by movements that stress an anulus fibrosus, associated with a history compatible with singular or cumulative injury to the anulus fibrosus. A history of activities or injury consistent with the affected anulus fibrosus having been strained. Partial or complete tears of the anulus fibrosus in a location consistent with the nature of the precipitating stress; typically: circumferential tears of the outer layers of the anulus fibrosus caused by excessive combined flexion and rotation of the affected segment. Pain arises either as a result of an inflammatory repair response to the injured collagen fibers or as a result of excessive strain imposed by activities of daily living on the remaining, intact collagen fibers of the anulus fibrosus, which alone are insufficient to sustain these loads within their accustomed, normal physiological limits. Remarks Any clinical test used to diagnose sprain of the anulus fibrosus should be shown to be valid and reliable. Such clinical tests as have been advocated for this condition (Farfan 1985) have not been assessed for validity. Pathology Periostitis as a result of repeated contact between the two bones, progressing to sclerosis of the contact sites of the two bones. Remarks the radiographic presence of a pseudarthrosis in a patient with spinal pain is insufficient grounds alone to justify the diagnosis. Relief of pain following infiltration of local anesthetic into the lesion is not necessarily attended by relief following surgical treatment. Clinical Features Lumbar spinal pain, with or without referred pain, that can be aggravated by movements that stress the affected spinal segment, accompanied by radiographic evidence of instability. Diagnostic Criteria No universally accepted criteria exist for the clinical or radiographic diagnosis of instability, but for this classification to be used, one of the sets of criteria proposed in the literature must be satisfied, such as those of Posner et al. Pathology Loss of stiffness in one or more of the elements of a lumbar motion segment that resist translation, rotation, or both. The pain presumably arises as a result of excessive stresses being imposed by movement on structures such as the ligaments, joints, or anulus fibrosus of the affected segment. Remarks No studies have revealed exactly what the source of pain is in unstable lumbar motion segments nor what the mechanism of pain production is. Clinical Features Lumbar, lumbosacral, or sacral spinal pain associated with midline tenderness over the affected interspinous space, the pain being aggravated by extension of that segment of the vertebral column. Page 186 therefore, offered only as one of association between lumbar spinal pain and demonstrable movement abnormalities. Consequently, the diagnosis can be sustained only if the radiographic criteria are strictly satisfied. At the time of writing, although such criteria have been enunciated, reservations have also been raised about the internal and external reliability of measurements made on radiographs of the type used to demonstrate instability (Shaffer et al. The consistency and accuracy of roentgenograms for measuring sagittal translation in the lumbar vertebral motion segment: an experimental model, Spine, 15 (1990) 741-750. Remarks this classification should not be used unless the diagnostic criterion is satisfied. The presence of a pars interarticularis defect on radiographs or nuclear scans in a patient with lumbar spinal pain is not sufficient evidence to justify this diagnosis, because pars interarticularis defects occur in about 7% of asymptomatic individuals (Moreton 1966) and therefore may be only a coincidental finding in a patient with lumbar spinal pain. For this classification to be used evidence must be brought to bear that the observed defect is not asymptomatic. Diagnostic Features Radiographic or other imaging evidence of a fracture of the sacrum. Diagnostic Features A presumptive diagnosis may be made on the basis of imaging evidence of a neoplasm that directly or indirectly affects one or other of the tissues innervated by sacral spinal nerves. Clinical Features Sacral spinal pain with or without referred pain, associated with pyrexia or other clinical features of infection. Diagnostic Features A presumptive diagnosis can be made on the basis of an elevated white cell count or other serological features of infection, together with imaging evidence of the presence of a site of infection in the sacrum or its adnexa. Diagnostic Features Imaging or other evidence of arthritis affecting the sacroiliac joints. Diagnostic Features Imaging or other evidence of metabolic bone disease affecting the sacrum, confirmed by appropriate serological or biochemical investigations and/or histological evidence obtained by needle or other biopsy. Usually deep and aching with "heaviness and numbness" in the leg from buttock to foot, associated with narrowing of the vertebral canal. Main Features Patients usually have a long history of gradually increasing lumbar spinal with referred pain in the buttocks or lower limbs, with or without radicular pain, aggravated by extension of the lumbar spine, or by sustained postures that involve accentuation of the lumbar lordosis (like prolonged standing), and by walking. Walking also produces overt or subtle neurological features in the lower limbs that range from sensations of heaviness or clumsiness to paresthesias, numbness, weakness, and temporary paralysis of the lower limbs. The onset of these neurological features may be measured in terms of a "walking distance," which diminishes as the condition progresses in severity. Associated Symptoms There may be paresthesias and bowel or bladder disturbance, or impotence. Signs and Laboratory Findings X-rays usually demonstrate diffuse severe degenerative disease with facet hypertrophy and a shallow anteroposterior diameter of the lumbar canal. Magnetic resonance imaging and electrodiagnostic studies can also be helpful in demonstrating the areas involved. The dilemma posed by this condition is the discrepancy between physical signs, which are usually not great, and the subjective complaints. Pathology Encroachment upon and narrowing of the vertebral canal as a whole or of multiple lateral recesses thereof by osteophytes of the zygapophysial joints or syndesmophytes of the intervertebral disks. Congenital narrowing of the vertebral canal may predispose to this condition insofar as symptoms may arise in the face of osteophytes and syndesmophytes that in other individuals would not cause significant encroachment. The mechanism of the neurological features is unknown but may involve constriction of the dural sac with obstruction of flow of the cerebrospinal fluid, or obstruction of venous blood flow in the vertebral canal, or direct compression of spinal nerve roots. Radicular pain may arise as a result of compression or other compromise of one or more nerve roots but there is no evidence that the constrictive effects of spinal stenosis cause spinal pain and referred pain. These latter forms of pain ostensibly arise from the disorders of one or more of the disks or zygapophysial joints whose osteophytic overgrowth coincidentally causes the stenosis. Spinal stenosis is characterized by an essentially global distribution of neurological symptoms in the lower limbs, and in this respect should be distinguished from radicular pain due to foraminal stenosis, in which the pathology is restricted to a single intervertebral foramen and as such does not encroach upon the vertebral canal as a whole. Differential Diagnosis Peripheral vascular claudication, sciatic nerve compression, osteoarthritis of hip or knee, retroperitoneal tumors, other tumor or abscess, prolapsed lumbar disk. Diagnostic Features Imaging evidence of a congenital vertebral anomaly affecting the sacrum. Although they may be associated with pain, the specificity of this association is unknown. This classification should be used only when the cause of pain cannot be otherwise specified, but should not be used to imply that the congenital anomaly is the actual source of pain. Clinical Features Sacral spinal pain with or without referred pain, together with features of the disease affecting the viscus or vessel concerned. Diagnostic Features Imaging or other evidence of the primary disease affecting an abdominal or pelvic viscus or vessel. Clinical Features Pain perceived in the region of the sacroiliac joint with or without referred pain into the lower limb girdle or lower limb itself. Selectively infiltrating the putatively symptomatic joint with local anesthetic completely relieves the patient of the pain. Presumably the pain is caused by excessive stresses being imposed on the ligaments of the sacroiliac joint as a result of some structural fault in the joint itself or as a result of the joint as a whole being subject to inordinate stresses. Remarks this category does not encompass sacroiliitis, ankylosing spondylitis, or seronegative spondylarthropathies that may be demonstrated by radionuclide imaging other forms of imaging or diagnosed by other means. While there are beliefs that such disorders can befall the sacroiliac joint, no clinical tests of laudable validity and reliability have been devised whereby this condition can be diagnosed. Diagnostic Features Sacral spinal pain for which no other cause has been found or can be attributed. Remarks this definition is intended to cover those complaints that for whatever reason currently defy conventional diagno- Page 191 of such a condition, however, in the absence of any overt inflammatory joint disease, is implied by a positive response to an intraarticular injection of local anesthetic. Until such time as appropriate clinical tests are demonstrated to be valid and reliable, any diagnosis of sacroiliac joint pain based exclusively on clinical examination must be held to be only presumptive. Diagnostic Features Coccygeal pain for which no other cause has been found or can be attributed. In some instances, a more definitive diagnosis might be attainable using currently available techniques, but for logistic or ethical reasons these may not have been applied. Diagnostic Criteria Complete relief of pain upon infiltration of the putatively symptomatic joint or joints with local anesthetic, provided that the injection can be shown to have been selective in that it has not infiltrated other structures that might constitute the actual source of pain. Pathology Unknown, but presumably involves sprain of the capsule of the affected joint. Diagnostic Features Radiographic or other imaging evidence of multiple fractures throughout the vertebral column. X1*R Infiltrating Neoplastic Disease of the Vertebral Column or Its Adnexa, Other than Primary or Metastatic Tumors. Diagnostic Features Imaging or other evidence of metabolic bone disease affecting multiple regions of the vertebral column.
Patients with a suspected diagnosis of Neisseria conjunctivitis should be referred to an ophthalmologist for aggressive management as it can quickly lead to vision loss secondary to corneal ulceration and perforation antibiotics given for sinus infection generic keftab 250mg without a prescription. Acute bacterial conjunctivitis has the classic symptoms of discomfort antibiotic resistant pneumonia cheap keftab 750mg overnight delivery, blurry vision antibiotics for uti ppt order keftab 375 mg online, and mucopurulent secretions with "sticky" eyelids upon awakening bacteria synonym keftab 375 mg generic. Staphylococcus aureus and Staphylococcus epidermidis are common etiologies of conjunctivitis in adults treatment for uti toddlers generic keftab 375 mg without prescription, while Streptococcus pneumonia and Haemophilus influenza tend to affect children antimicrobial resistance and antibiotic resistance order keftab 500mg visa. Chronic bacterial conjunctivitis occurs when symptoms last longer than four weeks with frequent relapses. The patient complains of sore eyelids and ocular discomfort with little discharge. Bacterial culture is usually needed to identify the organism responsible for patients with chronic bacterial conjunctivitis. Tearing results from lashes abrading the globe Irritation, burning, and foreign body sensation. It presents very similarly to acute bacterial conjunctivitis, though it may be seen as smoldering chronic conjunctivitis in some cases. The common symptoms include ocular irritation, scant mucopurulent discharge, glued eyelids upon awakening and blurred vision. Patients do not respond well or fully to typical antibiotics that are prescribed for acute bacterial conjunctivitis. Treatment includes erythromycin ophthalmic ointment and oral therapy with azithromycin (single one gram dose) or doxycycline (100 mg twice a day for 14 days) to clear the infection. Seasonal allergic conjunctivitis is often the most common type and it is related to specific environmental allergens. Symptoms include bilateral eye lacrimation, itching, and diffuse erythema (Figure 1). Large cobblestone papillae under the eyelid and chemosis may be present in severe cases. Over-the-counter oral antihistamines and topical histamine H1-Receptor antagonists can help alleviate symptoms. It presents with chronic itching, photophobia, blurred vision, discoloration of the periorbital area and a thick, clear, stringy discharge. Everting the eyelids may reveal large flat papillae in severe cases of giant papillary allergic conjunctivitis. If the cornea appears hazy, ulcerated or symptoms fail to improve, the patient should be referred to an ophthalmologist for treatment. Treatment initially includes frequent use of artificial tears throughout the day and nightly application of lubricant ointments. In general, if treatment beyond lubricants proves ineffective, the dry eye, the patient should be referred to an ophthalmologist. If blepharitis is suspected, the patient should be evaluated for seborrheic dermatitis that is associated with scalp or facial flaking, as well as rosacea, which is associated with redness and swelling on the nose or cheeks. Treatment is supportive care such as eyelid hygiene, lid massage and warm compresses. When a patient does not respond to supportive care, topical erythromycin or bacitracin ophthalmic ointment can be used. In severe cases, oral antibiotics such as doxycycline or tetracycline may be considered. Treatment consists of antibiotic eye drops and/or ointment to prevent infection, supportive care, cycloplegics and pain control. If symptoms do not improve within 48 hours, the patient should be referred to an ophthalmologist. Ophthalmologist referral is warranted if there is corneal involvement, history of blunt trauma, drainage, or persistent pain. Treatment consists of supportive care and artificial tears, but in some cases may require a short course of topical steroids. Congenital ptosis results from a malformed levator muscle, while acquired ptosis may be due to the gradual thinning or disinsertion of the levator aponeurosis. For congenital or acquired ptosis, surgery is performed to tighten the levator aponeurosis or resect the levator muscle. The third (oculomotor) cranial nerve innervates all the extraocular muscles except the lateral rectus and superior oblique. Etiologies of the third nerve palsy include ischemic cranial mononeuropathy, vasculitis, compression of the third nerve by an aneurysm, tumor, or uncal herniation and trauma. Magnetic resonance imaging of the brain with contrast is required when there is no obvious vascular risk factor. If symptoms are seen in young patients, or there is suspicion for an aneurysm, cerebral angiography may be necessary. Variable ptosis, or ptosis worse at the end of the day may be signs of ocular myasthenia. Myasthenia gravis and its ocular variant are autoimmune disorders of the neuromuscular junction. A thorough workup including an acetylcholine receptor antibody titer, edrophonium chloride testing, nerve stimulation and chest computed tomography to rule out thymoma should be done. Patients with myasthenia should be referred to neurology for appropriate treatment. Congenital esotropia is rare and occurs before the age of 6 months and accommodative esotropia occurs between two and four years of age. Uveitis is an inflammatory condition involving the uveal tract and can be classified as anterior uveitis and posterior. Nonocular symptoms such as back pain, joint stiffness, dysuria can occur if systemic disorders are the cause of uveitis. Floating inflammatory cells and protein in the anterior chamber are detectable with the slit lamp biomicroscope. Inflammatory cells within the vitreous are known to cause a hazy view of the fundus of the eye. Kaur, Larsen, Nattis Primary Care Approach to Eye Conditions 33 the primary care physician may see galignant eyelid tumors such as basal cell carcinoma, squamous cell carcinoma and melanoma. Basal cell carcinoma is the most common eyelid malignancy that appears in the lower and medial region and it appears as a pearly nodule. Basal cell carcinoma has a low potential to metastasize, but it can become locally invasive. Squamous cell carcinoma is less prevalent but more aggressive when compared to basal cell carcinoma. It is known to be an aggressive tumor and metastasis to the lungs, liver and bone. When examining the eye, the physician should always evert the eyelid to look for any kind of conjunctival involvement. Reduced color perception, monocular diplopia, and night-time glare are also common symptoms. The treatment of choice is surgical removal of the lens and placement of an intraocular lens implant. Approximately 99% of patients obtain improved vision and quality of life after cataract surgery. If retinal detachment is suspected, the family physician should perform a dilated fundoscopic examination to visualize the detachment. If retinal detachment is suspected, the patient should immediately be referred to an ophthalmologist. Treatment of retinal detachment usually consists of surgery using laser photocoagulation to seal the retinal tear, then reattachment of the retina to the retinal epithelium. Acute angleclosure glaucoma is a medical emergency in which the intraocular pressure rises rapidly, potentially leading to permanent vision loss within hours. Physical examination typically shows a mid-dilated pupil, cloudy cornea and conjunctival injection. Mechanical globe injuries occur when there is a full thickness rupture through the cornea and the sclera. Patients with mechanical globe injuries present with eye pain, tearing, redness and decreased vision after trauma to the affected eye. Ocular emergencies, if not recognized early, can lead to permanent vision loss and therefore warrant immediate attention. Some of the ocular emergencies include retinal detachment, acute angle-closure glaucoma, mechanical globe injuries and chemical injuries. Retinal detachment occurs when the neurosensory layer of the retina is separated from the retinal pigment epithelium. A plastic or metal eye shield should be placed over the affected eye and patient should be immediately referred to an ophthalmologist. The primary care physician should educate the patient not to increase the eye pressure by coughing or straining. Computed tomography of the orbits is needed to evaluate for intraocular foreign bodies and fractures. Removal of foreign bod(ies) and surgical repair by an ophthalmologist greatly reduces the risk of endophthalmitis if performed within the first 24 hours of injury. Patients usually present with severe eye pain, redness, tearing, photophobia and decreased vision (Figure 4). A thorough examination of the external eye is necessary; periocular burns should be identified and pH testing should be performed. The Roper-Hall classification system (Table 6) may be used to describe the extent of the injury. Treatment involves placement of topical anesthetic followed by copious ocular surface irrigation using saline solution. Following irrigation, antibiotic eye drops are necessary; steroid drops and cycloplegics may also be used in certain cases. Ocular surface burns need close follow up with an ophthalmologist as early and late scarring can occur, leading to compromise of the ocular anatomy and possible vision loss. A detailed history and physical will help tailor the differential diagnosis appropriately. The primary care physician should also be able to recognize the scenarios that warrant immediate referral to anophthalmologist. If we follow systematic evaluation and grading, Dry eye disease is one condition that can be practiced at all levels of ophthalmic care. Only cases of severe grades of dry eye and those with associated systematic disease, needs expert opinion as well as evaluation by other fraternities like Rheumatology. The preferred practice patterns on dry eye disease is first of its kind to give a global perspective pertinent to Indian Scenario in terms of management of dry eye disease. I would like to thank Dr Samar Kumar Basak for his efforts and Dr Virender S Sangwan & Namrata Sharma, for their expert comments on the subject. Dr Ajit Babu Majji Chairman, Academic & Research Committee All India Ophthalmological Society Medical Director, Centre For Sight Ashoka Capitol Building, Road# 2, Banjara Hills Hyderabad 500034, India E mail: ajitbabu2012@gmail. Due to a wide variety of presenting symptoms, it is often unrecognized and this causes great frustration of the patient and treating physician. While these symptoms often improve with appropriate treatment, usually in majority of the cases the disease may not be curable. In many cases, dry eye disease can be a cause of significant visual morbidity and may compromise the results of cataract, corneal and refractive surgery. There are great advances in the understanding of dry eye disease over the past 10-15 years in the area of epidemiology, pathogenesis, clinical manifestation, and possibly in the therapeutic regimen. These are on the articles published in the peer-review journals on different aspect on dry eye diseases, such as, epidemiology, inflammatory aspect, tears substitutes, surgical options, newer treatment options, etc. We strive to communicate effectively with our dry eye patients, listening carefully to their needs and concerns. This is important to ensure about their active participation in decisions affecting their management, to improve their motivation and compliance with the agreed therapeutic plan, and also to help alleviate their fears and concerns about the disease. Continuous 48 counselling in every visit is an important key factor to boost up the psychological status of the patients. Dr Samar K Basak Disha Eye Hospitals & Research Centre Barrackpore, Kolkata 700 120 West Bengal Tel: 0-9830323013 Email: basak sk@hotmail. In 1995: National Eye Institute/industry workshop: Consensus developed on definition, diagnosis and treatment. It is accompanied by increased osmolality of tear film and inflammation of the ocular surface. However, there are only three published reports on prevalence of dry eye among hospital-based population from North and Eastern India and the prevalence varies between 18. Target audience: Primary eye care physician/optometrists, resident/ fellow ophthalmologists, comprehensive ophthalmologists, ophthalmic private practitioners and all sub speciality ophthalmologists. Demography Epidemiology There is no doubt that in recent years, dry eye disease is an extremely common condition that causes varying degrees of ocular discomfort and disability. Thus, there has been a shift towards symptom-based assessment as the key component of clinical diagnosis. There are only three studies from India available in the peer-review journals and two of them from the North and one from Eastern India. With different diagnostic criteria the prevalence of dry eye in these studies was Between 18. Environmental factors, such as reduced humidity and increased wind, drafts, air conditioning, or heating may exacerbate the ocular discomfort. Exogenous irritants and allergens, although not believed to be causative of dry eye, may exacerbate the symptoms.
Screening in Dental Practices In the last decade bacteria battery discount 250 mg keftab mastercard, the incidence and prevalence of type 2 diabetes in adolescents has increased dramatically virus in michigan keftab 750mg on-line, especially in racial and ethnic minority populations (33) infection 7 months after hysterectomy cheap keftab 250mg on line. See Section 13 "Children and Adolescents" for additional information on type 2 diabetes in children and adolescents antibiotics joke keftab 375mg online. However antibiotics for uti caused by e coli generic keftab 250mg without a prescription, many of these studies do not recognize that diabetes diagnostic criteria are based on long-term health outcomes oral antibiotics for acne during pregnancy 250 mg keftab fast delivery, and validations are not currently available in the pediatric population (63). The ongoing epidemic of obesity and diabetes has led to more type 2 diabetes in women of childbearing age, with an increase in the number of pregnant women with undiagnosed type 2 diabetes (66). Because of the number of pregnant women with undiagnosed type 2 diabetes, it is reasonable to test women with risk factors for type 2 diabetes (67) (Table 2. Those trials found modest benefits including reduced rates of large-for-gestationalage births and preeclampsia (77,78). Treatment of higherthreshold maternal hyperglycemia, as identified by the two-step approach, reduces rates of neonatal macrosomia, large-for-gestational-age births (85), and shoulder dystocia, without increasing small-for-gestational-age births. Future Considerations the conflicting recommendations from expert groups underscore the fact that there are data to support each strategy. Data comparing population-wide outcomes with onestep versus two-step approaches have been inconsistent to date (91,92). Diabetes in this population, compared with individuals with type 1 or type 2 diabetes, is associated with worse nutritional status, more severe inflammatory lung disease, and greater mortality. In most cases, such stress- or steroidinduced hyperglycemia resolves by the time of discharge (106,107). Insulin therapy is the agent of choice for the management of hyperglycemia and diabetes in the hospital setting. After discharge, patients with preexisting diabetes could go back on their pretransplant regimen if they were in good control before transplantation. Drug dose adjustments may be required because of decreases in the glomerular filtration rate, a relatively common complication in transplant patients. A small short-term pilot study reported that metformin was safe to use in renal transplant recipients (114), but its safety has not been determined in other types of organ transplant. Thiazolidinediones have been used successfully in patients with liver and kidney transplants, but side effects include fluid retention, heart failure, and osteopenia (115,116). Dipeptidyl peptidase 4 inhibitors do not interact with immunosuppressant drugs and have demonstrated safety in small clinical trials (117,118). For a comprehensive list of causes, see Genetic Diagnosis of Endocrine Disorders (119). It is inherited in an autosomal dominant pattern with abnormalities in at least 13 genes on different chromosomes identified to date. In most cases, the presence of autoantibodies for type 1 diabetes precludes further testing for monogenic diabetes, but the presence of autoantibodies in patients with monogenic diabetes has been reported (121). Readily available commercial genetic testing following the criteria listed below now enables a cost-effective (122), often cost-saving, genetic diagnosis that is increasingly supported by health insurance. It is critical to correctly diagnose one of the monogenic forms of diabetes because these patients may be incorrectly diagnosed with type 1 or type 2 diabetes, leading to suboptimal, even potentially harmful, treatment regimens and delays in diagnosing other family members (124). Evaluation and management of youth-onset type 2 diabetes: a position statement by the American Diabetes Association. Impact of common genetic determinants of hemoglobin A1c on type 2 diabetes risk and diagnosis in ancestrally diverse populations: a transethnic genome-wide metaanalysis. Racial differences in glycemic markers: a cross-sectional analysis of community-based data. Racial and ethnic differences in mean plasma glucose, hemoglobin A1c, and 1,5-anhydroglucitol in over 2000 patients with type 2 diabetes. Hei moglobin A1c versus oral glucose tolerance test in postpartum diabetes screening. Is early postpartum HbA1c an appropriate risk predictor after pregnancy with gestational diabetes mellitus? Association between iron deficiency and A1C levels among adults without diabetes in the National Health and Nutrition Examination Survey, 1999-2006. Prognostic implications of singlesample confirmatory testing for undiagnosed diabetes: a prospective cohort study. Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. Identifying adults at high risk for diabetes and cardiovascular disease using hemoglobin A1c National Health and Nutrition Examination Survey 2005-2006. HbA1c as a predictor of diabetes and as an outcome in the Diabetes Prevention Program: a randomized clinical trial. National diabetes statistics report: estimates of diabetes and its burden in the United States, 2017 [Internet]. Association of gestational diabetes with maternal disorders of glucose metabolism and childhood adiposity. CarpenterCoustan compared with National Diabetes Data Group criteria for diagnosing gestational diabetes. The impact of adoption of the international association of diabetes in pregnancy study group criteria for the screening and diagnosis of gestational diabetes. Sensitivity and specificity of different methods for cystic fibrosis-related diabetes screening: is the oral glucose tolerance test still the standard? Short-term efficacy and safety of sitagliptin treatment in longterm stable renal recipients with new-onset diabetes after transplantation. Sitagliptin therapy in kidney transplant recipients with new-onset diabetes after transplantation. Population-based assessment of a biomarker-based screening pathway to aid diagnosis of monogenic diabetes in youngonset patients. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetesd2019 Diabetes Care 2019;42(Suppl. E Screening for prediabetes and type 2 diabetes risk through an informal assessment of risk factors (Table 2. See Section 2 "Classification and Diagnosis of Diabetes" and Section 6 "Glycemic Targets" for additional details on the appropriate use of the A1C test. Prevention or delay of type 2 diabetes: Standards of Medical Care in Diabetesd2019. The goal for physical activity was selected to approximate at least 700 kcal/ week expenditure from physical activity. For ease of translation, this goal was described as at least 150 min of moderateintensity physical activity per week similar in intensity to brisk walking. Nutrition Structured behavioral weight loss therapy, including a reduced calorie meal plan and physical activity, is of paramount importance for those at high risk for developing type 2 diabetes who have overweight or obesity (1,7). Because weight loss through lifestyle changes alone can be difficult to maintain long term (4), people being treated with weight loss therapy should have access to ongoing support and additional therapeutic options (such as pharmacotherapy) if needed. Additional research is needed regarding whether a low-carbohydrate eating plan is beneficial for persons with prediabetes (12). Whereas overall healthy low-calorie eating patterns should be encouraged, there is also some evidence that particular dietary components impact diabetes risk in observational studies. Higher intakes of nuts (16), berries (17), yogurt (18,19), coffee, and tea (20) are associated with reduced diabetes risk. Conversely, red meats and sugar-sweetened beverages are associated with an increased risk of type 2 diabetes (13). As is the case for those with diabetes, individualized medical nutrition therapy (see Section 5 "Lifestyle Management" for more detailed information) is effective in lowering A1C in individuals diagnosed with prediabetes (21). Physical Activity Just as 150 min/week of moderateintensity physical activity, such as brisk walking, showed beneficial effects in those with prediabetes (1), moderateintensity physical activity has been shown to improve insulin sensitivity and reduce abdominal fat in children and young adults (22,23). In addition to aerobic activity, an exercise regimen designed to prevent diabetes may include resistance training (6,24). Breaking up prolonged sedentary time may also be encouraged, as it is associated with moderately lower postprandial glucose levels (25,26). Technology-Assisted Interventions to Deliver Lifestyle Interventions are promising (39). Such technology-assisted interventions may deliver content through smartphone and web-based applications and telehealth (28). The selection of an in-person or virtual program should be based on patient preference. Cost-effectiveness Smoking may increase the risk of type 2 diabetes (40); therefore, evaluation for tobacco use and referral for tobacco cessation, if indicated, should be part of routine care for those at risk for diabetes. Metformin has the strongest evidence base (50) and demonstrated long-term safety as pharmacologic therapy for diabetes prevention (48). Consider monitoring vitamin B12 levels in those taking metformin chronically to check for possible deficiency (54) (see Section 9 "Pharmacologic Approaches to Glycemic Treatment" for more details). B People with prediabetes often have other cardiovascular risk factors, including hypertension and dyslipidemia (55), and are at increased risk for cardiovascular disease (56). Although treatment goals for people with prediabetes are the same as for the general population (57), increased vigilance is warranted to identify S32 Prevention or Delay of Type 2 Diabetes Diabetes Care Volume 42, Supplement 1, January 2019 and treat these and other cardiovascular risk factors. B As for those with established diabetes, the standards for diabetes self-management education and support (see Section 5 "Lifestyle Management") can also apply to people with prediabetes. Although reimbursement remains a barrier, studies show that providers of diabetes self-management education and support are particularly well equipped to assist people with prediabetes in developing and maintaining behaviors that can prevent or delay the development of diabetes (21,58). Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: a 23-year follow-up study. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the Diabetes Prevention Program Outcomes Study. Protective effects of the Mediterranean diet on type 2 diabetes and metabolic syndrome. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. Longterm low-carbohydrate diets and type 2 diabetes risk: a systematic review and meta-analysis of observational studies. A priori-defined diet quality indexes and risk of type 2 diabetes: the Multiethnic Cohort. Consumption of nuts and legumes and risk of incident ischemic heart disease, stroke, and diabetes: a systematic review and meta-analysis. Effects of aerobic training, resistance training, or both on percentage body fat and cardiometabolic risk markers in obese adolescents: the healthy eating aerobic and resistance training in youth randomized clinical trial. Diabetes prevention: interventions engaging community health workers [Internet], 2016. Long-term safety, tolerability, and weight loss associated with metformin in the Diabetes Prevention Program Outcomes Study. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetesd2019 Diabetes Care 2019;42(Suppl. E A successful medical evaluation depends on beneficial interactions between the patient and the care team. People with diabetes should receive health care from an interdisciplinary team that may include physicians, nurse practitioners, physician assistants, nurses, dietitians, exercise specialists, pharmacists, dentists, podiatrists, and mental health professionals. The patient, family or support people, physicians, and health care team should together formulate the management plan, which includes lifestyle management (see Section 5 "Lifestyle Management"). The goals of treatment for diabetes are to prevent or delay complications and maintain quality of life (Fig. Treatment goals and plans should be created Suggested citation: American Diabetes Association. Comprehensive medical evaluation and assessment of comorbidities: Standards of Medical Care in Diabetesd2019.
Discount keftab 500 mg mastercard. 10 Best Home Remedies for Treating Candida Yeast Infections.