X



|
STUDENT DIGITAL NEWSLETTER ALAGAPPA INSTITUTIONS |

|
Genevieve Guenther Ricart Embree, MD

https://medicine.duke.edu/faculty/genevieve-guenther-ricart-embree-md
Once about twothirds to three-fourths of nutrient needs can be provided enterally medications 142 proven 10mg endep, the intravenous feedings may be discontinued treatment kidney cancer symptoms buy endep 25 mg free shipping. Patients receiving continuous parenteral feedings may have better appetites during the day if they are switched to nocturnal cyclic feedings before beginning oral intakes treatment 5 alpha reductase deficiency generic 10 mg endep mastercard. Managing Metabolic Complications As has been discussed symptoms you need glasses cheap endep 10mg with visa, the catheters used for parenteral nutrition may cause a number of serious complications. This section describes some metabolic complications that may result from parenteral feedings (review Table 21-2) and some suggestions for managing them. It can be prevented by providing insulin along with feedings or by restricting the amount of dextrose in a solution. Dextrose infusions are generally limited to less than 5 milligrams per kilogram of body weight per minute in critically ill adult patients so that the carbohydrate intake does not exceed the maximum glucose oxidation rate. Premature infants are especially likely to develop hyperglycemia, because their pancreas and liver are not fully functioning. Hypoglycemia Although uncommon, hypoglycemia sometimes occurs when feedings are interrupted or discontinued or if excessive insulin is given. In patients at risk, such as young infants, feedings may be tapered off over several hours before discontinuation. Another option is to infuse a 10 percent dextrose solution at the same time that the parenteral feedings are interrupted or stopped. Patients at risk include those with severe infection, liver disease, kidney failure, hyperglycemia, and use of immunosuppressant or corticosteroid medications. If blood triglyceride levels exceed 500 milligrams per deciliter, lipid infusions should be reduced or stopped. These effects occur because dextrose infusions raise circulating insulin levels, which promote anabolic processes that quickly remove phosphate, potassium, and magnesium from the blood. The altered electrolyte levels can lead to fluid retention and life-threatening changes in organ systems. Refeeding syndrome generally develops within two weeks of beginning parenteral feedings. To prevent refeeding syndrome, health practitioners start parenteral feedings slowly and carefully monitor electrolyte and glucose levels when malnourished patients begin receiving nutrition support. Abnormal Liver Function Fatty liver often results from parenteral support, but it is usually corrected when the parenteral feedings are discontinued. Long-term parenteral nutrition, however, may result in chronic, irreversible liver disease that can eventually lead to liver failure. Liver enzyme levels are monitored weekly during parenteral support, and abnormal values are often seen within weeks of beginning the feedings. Some amount of enteral intake may be encouraged to reduce the amount of parenteral support necessary. Note that various critical illnesses and disease treatments can also cause liver complications, so parenteral nutrition cannot be assumed to be the underlying cause. When parenteral nutrition continues for more than four weeks, sludge (thickened bile) often builds up in the gallbladder and may eventually lead to gallstone formation. Prevention is sometimes possible by initiating enteral feedings before problems develop. Patients requiring long-term parenteral nutrition may be given cholecystokinin injections to cause gallbladder contraction and bile release or may have their gallbladders removed surgically. Metabolic Bone Disease Long-term parenteral nutrition has been associated with lower bone density and bone mineralization, which may be related to altered calcium, phosphorus, magnesium, and sodium metabolism. Imbalanced intakes of vitamin D, vitamin K, and phosphorus have also been implicated. Therefore, nutrition status and bone density are routinely monitored during long-term parenteral nutrition. The ideal intervention for metabolic bone disease varies among patients; it may include dietary adjustments, nutrient supplements, medications, and physical activity. Parenteral solutions may be initiated gradually or provided at full volume and full strength in selected patients. Critically ill patients may require continuous feedings, whereas healthier patients and longterm users may prefer cyclic feedings. Catheters are frequently the cause of complications, which include improper placement or dislodgment, infection, clotting, embolism, and phlebitis. Metabolic complications include hyperglycemia and hypoglycemia; hypertriglyceridemia; fluid and electrolyte imbalances; and diseases affecting the liver, gallbladder, and bone. When the need for parenteral nutrition resolves, patients are transitioned to an enteral diet as the volume of parenteral nutrition is gradually reduced. The Case Study can be used to check your understanding of the concepts introduced in this chapter. Nutrition Support at Home Occasionally, a patient must continue to receive nutrition support, either tube feedings or parenteral nutrition, after a medical condition has stabilized. Current technology allows for the safe administration of nutrition support in home settings, and insurance coverage often pays a substantial portion of the costs. Home health services and home infusion pharmacies can provide the equipment, enteral formulas or parenteral solutions, and services necessary for home nutrition care. Most important, patients using these services can continue to receive specialized nutrition care while leading normal lives. Candidates for Home Nutrition Support Individuals referred for home nutrition support usually need long-term nutrition care for chronic medical conditions. Users of home nutrition services (or their families and other caregivers) must be intellectually capable of learning the necessary procedures, monitoring the treatment, and managing complications as necessary. After 10 days, tube feeding was begun, which initially delivered very small feedings. Calculate the energy content of 1 liter of a solution that provides 140 grams of dextrose monohydrate, 45 grams of amino acids, and 90 milliliters of 20 percent lipid emulsion. Assuming that Jerry eventually tolerates a tube feeding, in what ways can the health care team help Jerry make the transition from parenteral feedings to tube feedings? Consider some of the physiological problems that Jerry might face when he begins eating an oral diet. As you read through the section on nutrition support at home, consider the factors that would make Jerry a good candidate for a home nutrition support program. Consider both the benefits of a proposed program and the problems he could encounter. The costs should be clearly explained to families who cannot get insurance reimbursement. Examples include patients with head and neck cancers and individuals with neurological impairments that cause difficulties with swallowing. Examples include persons who have had large portions of their small intestine removed and those with intestinal obstructions or malabsorption conditions. Planning Home Nutrition Care As with the nutrition support provided in health care facilities, planning for home nutrition care involves decisions about access sites, formulas, and nutrient delivery methods. Users of home services should be involved in the decision making to ensure long-term compliance and satisfaction. People sometimes learn to place nasogastric tubes themselves, which may improve acceptance of the therapy. Active children and adults often prefer low-profile gastrostomy tubes, which allow them to lead a more normal lifestyle. Jejunostomy tubes may be required for some individuals but are less convenient, because the frequent feedings required for people with jejunostomies can interfere with daytime activities. Insurance reimbursements do not always include the cost of formula, which is considered to be a "food" product. Blenderizing home-cooked foods is possible, but the foods need to be strained to remove particles and clumps that may obstruct the tube. Closed (ready-to-hang) feeding systems are useful for avoiding contamination risk Portable pumps and convenient carrying cases allow people who require nutrition support at home to move about freely. The advantages and disadvantages associated with the different administration methods should be fully discussed with patients. Gravity drip infusions eliminate the need for an infusion pump, but the delivery rates are less reliable. If intermittent feedings are appropriate, they should be tailored to daily routines. Portable pumps can free individuals from the need to infuse formula at home and can also be used when traveling. The catheter can be inserted so that the exit site is in a region that is accessible to the patient.
Diseases
Treating stage 0 rectal cancer Stage 0 rectal cancers have not grown beyond the inner lining of the rectum treatment lead poisoning buy 25 mg endep visa. You can usually be treated with surgery such as a polypectomy (removing the polyp) medications versed buy cheap endep 50 mg on line, local excision medicine river cheap 75 mg endep amex, or transanal resection treatment wpw cheap endep 75mg free shipping. Treating stage I rectal cancer Stage I rectal cancers have grown into deeper layers of the rectal wall but have not spread outside the rectum itself. If the polyp is removed completely during colonoscopy, with no cancer in the edges, no other treatment may be needed. If the cancer in the polyp was high grade (see Colorectal Cancer Stages2), or if there were cancer cells at the edges of the polyp, you might be advised to have more surgery. Some small stage I cancers can be removed through the anus without cutting the abdomen (belly), using 46 American Cancer Society cancer. If it is more advanced, a combination of chemo and radiation therapy is usually given. Additional chemo is then given after surgery, usually for a total of about 6 months. Most often, chemo is given along with radiation therapy (called chemoradiation) first. Giving radiation before surgery also tends to lead to fewer problems than giving it after surgery. If the cancer has reached nearby organs, a more extensive operation known as pelvic exenteration may be needed. Another option might be to get chemotherapy alone first, followed by chemo plus radiation therapy, then followed by surgery. Chemoradiation, followed by surgery to remove the rectal cancer and distant cancer. If not, the cancer will likely be treated with chemo and/or targeted therapy drugs (without surgery). If chemo shrinks the cancer, in some cases it may be possible to consider surgery to try to remove all of the cancer at this point. For people with certain gene changes in their cancer cells, another option after initial chemotherapy might be treatment with an immunotherapy drug such as pembrolizumab (Keytruda) or nivolumab (Opdivo). Treating recurrent rectal cancer Recurrent cancer means that the cancer has come back after treatment. It may come back near the area of the initial rectal cancer (locally) or in distant organs, like the lungs or liver. In some cases radiation therapy may be given during the surgery (this is called intraoperative 50 American Cancer Society cancer. Distant recurrence If the cancer comes back in a distant part of the body, the treatment will depend on whether it can be removed by surgery. When the cancer has spread to the liver, chemo may be given through the hepatic artery leading to the liver. For people with certain gene changes in their cancer cells, another option might be treatment with immunotherapy. The drugs used will depend on what drugs a person has received previously and on their overall health. These cancers can often be hard to treat, so you might also want to ask your doctor if there are any clinical trials3 of newer treatments that might be right for you. The treatment information given here is not official policy of the American Cancer Society and is not intended as medical advice to replace the expertise and judgment of your cancer care team. Last Revised: June 29, 2020 Written by the American Cancer Society medical and editorial content team ( Esophageal Cancer Risk Factors A risk factor is anything that increases your chance of getting a disease such as cancer. Scientists have found several factors that can affect your risk of esophageal cancer. But having a risk factor, or even many, does not mean that you will get esophageal cancer. Tobacco and alcohol the use of tobacco products1, including cigarettes, cigars, pipes, and chewing tobacco, is a major risk factor for esophageal cancer. The more a person uses tobacco and the longer it is used, the higher the cancer risk. Someone who smokes a pack of cigarettes a day or more has at least twice the chance of getting adenocarcinoma of the esophagus than a nonsmoker, and the risk does not go away if tobacco use stops. The link to squamous cell esophageal cancer is even stronger, but this risk does go down for people who quit tobacco. The more alcohol someone drinks, the higher their chance of getting esophageal cancer. Alcohol increases the risk of squamous cell carcinoma more than the risk of adenocarcinoma. Smoking combined with drinking alcohol raises the risk of the squamous cell type of esophageal cancer much more than using either alone. Gastroesophageal reflux disease the stomach normally makes strong acid and enzymes to help digest food. In some people, acid can escape from the stomach up into the lower part of the esophagus. In many people, reflux causes symptoms such as heartburn or pain that seem to come from the 2 American Cancer Society cancer. This causes the squamous cells that normally line the esophagus to be replaced with gland cells. These gland cells usually look like the cells that line the stomach and the small intestine, and are more resistant to stomach acid. Low-grade dysplasia looks more like normal cells, while high-grade dysplasia is more abnormal. Obesity People who are overweight or obese3 (very overweight) have a higher chance of getting adenocarcinoma of the esophagus. This is in part explained by the fact that people who are obese are more likely to have gastroesophageal reflux. For example, there have been suggestions, as yet not well proven, that a diet high in processed meat may increase the chance of developing esophageal cancer. The exact reasons for this are not clear, but fruits and vegetables have a number of vitamins and minerals that may help prevent cancer. Frequently drinking very hot liquids (temperatures of 149° F or 65° C - much hotter than a typical cup of coffee) may increase the risk for the squamous cell type of esophageal cancer. This might be the result of long-term damage to the cells lining the esophagus from the hot liquids. Physical Activity People who engage in regular physical activity may have a lower risk of adenocarcinoma of the esophagus. Achalasia In this condition, the muscle at the lower end of the esophagus (the lower esophageal sphincter) does not relax properly. Food and liquid that are swallowed have trouble passing into the stomach and tend to collect in the lower esophagus, which becomes stretched out (dilated) over time. The cells lining the esophagus in that area can become irritated from being exposed to foods for longer than normal amounts of time. Tylosis this is a rare, inherited disease that causes extra growth of the top layer of skin on the palms of the hands and soles of the feet. People with this condition also develop small growths (papillomas) in the esophagus and have a very high risk of getting squamous cell cancer of the esophagus. People with tylosis need to be watched closely to try to find esophageal cancer early. Often this requires regular monitoring with an upper endoscopy (described in Tests for Esophagus cancer)4. Plummer-Vinson syndrome People with this rare syndrome (also called Paterson-Kelly syndrome) have webs in the 4 American Cancer Society cancer. A web is a thin piece of tissue extending out from the inner lining of the esophagus that causes an area of narrowing. Most esophageal webs do not cause any problems, but larger ones can cause food to get stuck in the esophagus, which can lead to problems swallowing and chronic irritation in that area from the trapped food.
They present emotional or physical issues for which the biomedical modality has been limited or dissatisfying in some way medicine 8 capital rocka discount 75 mg endep mastercard, and find success with the application of neo-shamanic healing techniques treatment concussion 75 mg endep with amex. Although it can result in a very practical resolution of physical symptoms and conditions doctor of medicine safe 75mg endep, it does so on the premise of an enchanted cosmology medications memory loss generic endep 50mg overnight delivery. Priorities shift from attaining a measurable physical change, as required by the disenchanted, material premise of biomedicine, to becoming aware, empowered, and integrated-in one word: transformed. However, here the tension between a healing system premised on a traditional, premodern sense of the universe and the people using it who are embodying the modern self becomes manifest anew. People struggle to explain their lived experiences premised on an enchanted world exterior to the self. And they put these experiences into the language of a healing terminology that fits with modern society, one that presents nonordinary (shamanic) experience as internal, not extramaterial, as premised by the ideas of shamanism. For this reason, shamanic healing is often couched in terms of "interior experience" and not validated as a legitimate, external, healing modality. This dissertation takes a critical approach to the structure of modernity, following Weber: that is, the modern emphasis on the external, material, and measurable disenchants the world and the result is a Western worldview that is ontologically deficient. Neo-shamanism draws its worldview from a premodern structure, that is, a structure that emphasizes the animated, enchanted, and collective (social), a structure in which meaning is assumed to be available. However, although premised on what are considered to be premodern ideas about the nature of being, neo-shamanism is at its essence oriented on the self, thus it is a truly modern engagement with an ostensibly "traditional" enchanted cosmos. His premise is that the "enlightened" Cartesian differentiation of matter and spirit, which is taken as the hallmark of the modern era, is an illusion. To be strictly modern, we must ignore what does not fit neatly into the separate categories of matter and spirit, mundane and sacred, nature and culture. He argues that as moderns we can only pretend to uphold this strict division, because we must simultaneously live in a world where, frankly, the division does not hold. Latour (1993) calls this the middle and is where people actually live their lives. Everything happens in the middle, everything passes between the two, everything happens by way of mediation, translation and networks, but this space does not exist, it has no place. And so, enchanted experience finds no place in the structure of modernity, yet modern individuals, because they are individuals, find no place in the collective structure of the traditional cultures from which the premises of neo-shamanism are drawn. Neo-shamanism is, thus, the stretching and re-shaping of traditional shamanism into something new. This is akin to the "complicated intercultural zone" Sahlins (1993:13) discusses in his article "Goodbye to Tristes Tropes. That is to say, novel items and ideas are pressed into the service of Own culture: foreign commodities serve to enrich native self-conceptions, they use them to create "their own culture on a bigger and better scale" (Sahlins 1993: 17). This has always been a function of culture, and is exactly what practitioners and participants of modern shamanism are doing: traditional shamanism arrives at the doorstep of modern culture, but before it can come in it must be transformed in a way that serves modernity and fits into it. Just as traditional societies indigenize modernity when they press novel items into the service of 174 their own culture, modern individuals press traditional shamanism into the service of themselves, resulting in an enchanted modernity. The key element of my thesis is that neo-shamanism is a contemporary cultural phenomenon in which traditional shamanic techniques and ideas are transformed into a constellation of techniques, practices, and beliefs about the nature of illness and the best way to heal it. It is a reworking of traditional shamanism in a modern context, for modern individuals, that is, for the "self. They turn foreign goods to the service of domestic ideas, to the objectification of their own relations and notions of the good life. Neo-shamanism can be considered from this perspective, not as a bastardization of some idealized form of traditional shamanism, but as a cultural phenomenon in its own right-one that offers a way to enchant modernity. While neo-shamanism is criticized as being frivolous and imaginary and largely ignored by the academe because "it is thought to be 175 harmless or irrelevant or downplayed because it is eccentric, fringe and laughable, of not interest to serious scholarship" (Wallis 2000: 260), this research demonstrates that modern shamanism is a serious undertaking of some individuals. It provides healing of a type not available in the medical institutions of modernity. Additionally, I argue that the most productive perspective from which to study a cultural phenomenon that takes people back and forth between the modern premises of their society and their enchanted lived personal experiences is that of experiential engagement. There is much yet to be investigated concerning neo-shamanism both in general and as a healing system alternative to biomedicine. The research reported here opens the door to further interest in and investigation of healing in modern society: where biomedicine and contemporary psychotherapy fall short and how people seek to answer their need for meaning, holism, and healing beyond the physical. Harner translated what he considered (nearly) universal traditional shamanic elements into an acultural package of practices for the modern shamanic seeker and participant. Detraditionalized Self: A term used to refer to the "modern self," in contrast to the traditional (premodern) individual. Disenchantment/Enchantment/Re-enchantment: Weber (1946) suggested that modernity disenchanted the world, i. Neo-shamanism, ostensibly based on traditional (premodern) shamanism, rests on the premise of an enchanted world, and neo-shamanic participants may find their world becomes re-enchanted as a result of their engagement with such. Experiential Participation: A research method in which the researcher approaches the study of unseen (to outsiders) experiences by personally engaging in those experiences. Extra-material: An unseen (or spiritual) realm external to self for which (neo)shamans employ an altered state of consciousness to apprehend. The (neo)shamanic practitioner locates these intrusions and extracts them, disposing of them in a way that will neutralize their negative energy, like sending them to a body of water, placing them in fire, or burying them in the ground. Limited Holism: the phrase Baer (2003) uses to refer to a holism which emerged out of the Holistic Health movement, in which the focus on individual responsibility for health disregards society and its institutions as factors in illness, providing an "alternative form of medical hegemony by reinforcing individualizing patterns in U. While mesa is a specific cultural term referring to the spiritual altar of the traditional Northern Peruvian shamanic practitioner as described by Glass-Coffin (1998) and Joralemon and Sharon (1993), it is used in this dissertation to refer to any dedicated, animated curing space or altar used by modern shamanic practitioners and participants. Neo-shamanism: Neo-shamanism is the application and practice of shamanic techniques in contemporary Western society and functions as a system of healing alternative to biomedicine. It is also sometimes called contemporary shamanism, American shamanism, and modern shamanism. Nonordinary Reality: See "extra-material" Participant-observation: the combination of participating in the daily life of the culture or group being researched while at the same time observing and recording observations. Shamanic Journey: the seminal neo-shamanic tool: it entails accessing an altered state of consciousness, usually through auditory driving (drumming or rattling) while sitting still or lying down, in which the shamanic practitioner travels into nonordinary reality in order to get information for healing. This may be akin to "seeing" an aura around a person, place, or object, or to "hearing" information about someone or some thing. Soul Loss/Soul Retrieval: A cross-cultural shamanic disease category and therapeutic modality: an individual can lose part of his or her soul (thus his or her vital essence) as a result of trauma or interpersonal relationships. Symptoms associated with soul loss are depression, fatigue, a feeling that part of self is missing, addiction, chronic disease, and immune deficiency problems. Andrews the Four Fold Way: Walking the Paths of the Warrior, Teacher, Healer, and Visionary by Angeles Arrien, PhD Satsun: My Apprenticeship with a Maya Healer by Rosito Arvigo with Nadine Epstein Black Elk: the Sacred Ways of a Lakota by Wallace Black Elk and William S. Bruce Lamb Extraordinary Knowing: Science, Skepticism, and the Inexplicable Powers of the Human Mind by Elizabeth Lloyd Mayer, PhD the Archaic Revival by Terrance McKenna Mutant Message Down Under by Marlo Morgan Urban Shaman (trilogy) by C. Studying Machupe Shaman/Healers in Chile from an Experiential Perspective: Ethical and Methodological Problems. The Work of Andrew Weil and Deepak Chopra-Two Holistic Health/New Age Gurus: A Critique of the Holisitc Health/New Age Movements. Complementary and Alternative Medicine Use Among Adults and Children: United States, 2007. Research Methods in Anthropology: Qualitative and Quantitative Approaches, 2nd edition. Firewalking and Religious Healing: the Anastenaria of Greece and the American Firewalking Movement. On Medicine Women and White Shame-Ans: New Age Native Americananism and Commodity Fetishism as Pop Culture Feminism. The Health Consequences of Cultural Consonance: Cultural Dimensions of Lifestyle, Social Support, and Arterial Blood Pressure in an African American Community. Unconventional Medicine in the United States-Prevalence, Costs, and Patterns of Use. Electric Body, Magnetic Mind, Trance Healing and Shamanic Freedom: the Resacralization of the Human Body. Department of Sociology, Social Work, and 187 Anthropology, Utah State University, Logan, Utah. Shamanism: Traditional and Contemporary Approaches to the Mastery of Spirits and Healing. Taming the Wind of Desire: Psychology, Medicine, and Aesthetics in Malay Shamanistic Performance.
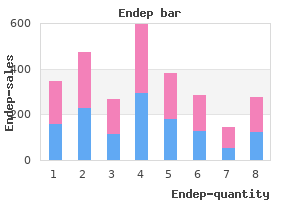
The names of the categories in the third column medications ending in ine proven 50mg endep, labeled "Damage symptoms walking pneumonia buy endep 50mg without prescription," could best be described as a 25 medications to know for nclex quality 75 mg endep. Which of the following incidents at Hanesboro Crossing would be considered an act of nature? A deer hunter lighting a cigarette accidentally tossed a match too close to a dry shrub medicine x ed generic endep 50mg on line. The status of the town with the most number of days without significant precipitation is a. The largest number of men in the Baidya caste of Madaripur are involved in which field? The smallest number of men in the Baidya caste of Madaripur are involved in which field? In which competition did Korea win an equal number of gold, silver, and bronze medals? Notice 1 All drivers are responsible for refueling their vehicles at the end of each shift. All other routine maintenance should be performed by maintenance department personnel, who are also responsible for maintaining service records. If a driver believes a vehicle is in need of mechanical repair, the driver should fill out the pink repair requisition form and give it to the shift supervisor. Because the length of time it takes to complete different tasks and routes vary, trucks within the same department will no longer be assigned to specific routes but will be rotated among the routes. Therefore, drivers should no longer leave personal items in the trucks, because they will not necessarily be driving the same truck each day, as they did in the past. According to the passage, prior to instituting the graffiti clean-up program, city workers a. Drivers are reminded that each route has several checkpoints at which drivers should check the time. If the bus is ahead of schedule, drivers should delay at the checkpoint until it is the proper time to leave. If traffic makes it unsafe for a driver to delay at a particular checkpoint, the driver should proceed at a reasonable speed to the next stop and hold there until the bus is back on schedule. If you are unclear whether a particular item is hazardous, you should not handle the item but should instead notify a supervisor of the Sanitation. Sanitation Worker Harris comes upon a container of cleaning solvent along with the regular garbage in front of a residence. Instructors who have used this new technology report that trainees develop skills more quickly than with traditional training methods. In refresher training, this new system reinforces defensive driving skills and safe driving habits. As an added benefit, the city expects to save money with the simulators, because the new system reduces the amount of training time in an actual bus-saving on parts, fuel, and other operating expenses. Classes will be taught on Monday afternoons, Wednesday evenings, and Saturday afternoons. These include completion of technician-level training and certification in hazardous material (hazmat) operations. In addition, after becoming a member, you must also attend a minimum of 50% of all drills conducted by F. You may qualify for alternative credit for drills by proving previous experience in actual hazmat emergency response. If you fail to meet minimum requirements, you will be considered inactive, and the director of your team will be notified. You will be placed back on active status only after you complete the training necessary to meet the minimum requirements. Please take time before that date to familiarize yourself with both the existing P&P and the planned changes. Certain changes may affect your job description, vacation time, medical benefits, or other aspects of employment. These changes will become effective beginning July 1, but will not be considered retroactive. Some areas that will change include the following: Overtime cap for hourly employees Sick time for salaried employees Safety requirements for yard workers Dress code for office employees If you have any questions concerning these changes, please contact the Human Resources office at ext. All employees will be expected to understand and abide by the new P&P statement, as defined on our website and in our employee handbook. A wind speed of 143 miles per hour falls between 113 and 157, which is the range for an F2 tornado, choice c. Choices a and b (F0 and F1) have lower wind speeds, while choice d (F3) has a higher wind speed. Applying words such as mild, moderate, significant, severe, devastating, incredible, and inconceivable to the damage done by a tornado is a means of describing the damage; therefore, the words are descriptive, choice b. The Voorhees Air fire (choice b) occurred on June 12, two days before the Cougar Run fire. The Murphy County Nature Reserve fire (choice c) occurred on June 13, one day before the Cougar Run fire. The Burgaw Grove fires (choice d) occurred on June 2 (12 days before the Cougar Run fire) and June 21 (one week after the Cougar Run fire). Moving on to the "Number of Acres Burned" column, the 115 acres at Burgaw Grove and 320 acres at Hanesboro Crossing add up to 435 acres-which is less than 500 acres (choice b). According to the chart, the arson fires consumed 526 acres (Stone River State Park) and 1,200 acres (Bramley Acres Resort)-1,726 acres total-which is more than the 435 acres consumed by lightning fires. If you look at the same row under the "Status" column, Parkston is identified as level three. This eliminates choices b and c, because now you know that Chase Crossing is not less likely to experience a fire, or equally as likely to experience a fire. Therefore, combining the number of students and teachers gives the largest number involved in education (79). Only 2 of the 200 men in the Baidya caste are farmers-fewer than any other occupation on the chart. There are 79 in education (choice a), 44 in government service (choice c), and 5 in publishing (newspapers and presses, choice d). If you look at the "Total" column, it shows you that China (choice a) had the most total medals with six; Korea (choice b) came next with three; and Denmark (choice c) was third with one. Denmark has zeroes in every column except "Bronze," so this is the correct answer. In the column for April, the average temperature row tells you that 23° (choice c) is the right number. To find the answer, look for where the March column and the Average Precipitation row intersect; this gives you 7. In the same row, you see that people with an income between $25,000 and $40,000 will pay 13% (choice d) in taxes. The chart lists income tax paid as a percentage, not a dollar amount-so $13 (choice b) and $13,000 are not correct. An income of $75,000 would put you in the "70100" range, which pays 5% in Social Security (choice a). The chart lists Social Security paid as a percentage, so $12,000 (choice b) is incorrect. None of the listed Social Security percentages are given as 18% (choice c) for any income range, so that is incorrect. The only income range that pays 0% Social Security is $0$15,000, which is far below the $75,000 amount given. For the $25,000$40,000 range (choice a), the income tax plus Social Security is 13 + 9, or 22% total. For the $20,000$25,000 range (choice b), the income tax plus Social Security is 12 + 7, or 19% total. For the $15,000$20,000 range (choice c), the income tax plus Social Security is 10 + 5, or 15% total-which matches the question. For the $0$15,000 range (choice d), the income tax plus Social Security is 0 + 0, or 0% total. An oil change is likely considered "routine maintenance," so the second sentence tells you that routine maintenance is the responsibility of maintenance department personnel (choice a).
Order endep 50mg without a prescription. Group B Strep in Pregnancy.