X



|
STUDENT DIGITAL NEWSLETTER ALAGAPPA INSTITUTIONS |

|
Stephen M. Rosenthal MD

https://profiles.ucsf.edu/stephen.rosenthal
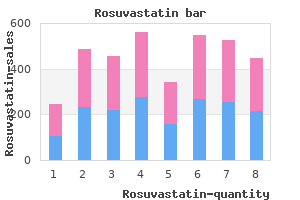
The Eastern Shore is highly agricultural and has the highest concentration of animal feeding operations (particularly broiler chicken operations) in the state (Dance natural cholesterol lowering foods herbs cheap rosuvastatin 10mg with visa, 2016; Environmental Integrity Project cholesterol new drug order 10mg rosuvastatin overnight delivery, 2015; T cholesterol high medication rosuvastatin 10 mg line. Montgomery County is also characterized by a large number of homes that rely on private wells; however cholesterol levels and stroke risk cheap 10 mg rosuvastatin amex, there are fewer animal feeding operations in this county. Participants were limited to homeowners in the aforementioned counties with private wells who were interested in participating in the clinics. The survey included questions on well characteristics, homeowner well management practices, prior testing conducted (if any), demographic questions (age, sex, race/ethnicity, and income level), and general health-related questions, including, "In the past month, have you experienced diarrhea Following completion of laboratory analyses (described below), a second follow-up clinic was held where water quality results were returned to participants who provided water samples. The results were individually and confidentially interpreted for participants and potential solutions for wells that did not meet federal standards were discussed where necessary. A followup survey was sent to all participants within 12 months after the clinics were 56 conducted to document actions taken by well owners to solve water quality problems or improve the management of their water supply as a result of attending our clinics (data not shown). The filters were then placed on the appropriate selective media for each microorganism. Positive and negative controls were used during each test, and plate counts were performed immediately after incubations. Specifically, we obtained data on the number of animal feeding operations with sales by zip code for the following animal types: 1) broiler chickens, 2) turkeys, 3) aquaculture, 4) sheep, 58 5) goats, 6) hogs, 7) dairy cattle, or beef cattle. We also linked well water data and animal feeding operation data by zip code and used univariate logistic regression models to evaluate associations between the presence of each type of animal feeding operation and detection of indicator bacteria in well water samples. The presence of total coliform bacteria and fecal coliform bacteria were the dichotomous (presence/absence) outcome variables of interest. However, only 118 participants returned both a water sample and a completed survey (Table 2). Approximately 12% and 0% of participants experienced diarrhea and vomiting, respectively, within 30 days prior to completing the survey. Regarding chemical contaminants, 26% of tested wells did not meet the recommended drinking water standard for pH (Figure 3), with most of these (83. Enterococcus was detected in samples from all counties; however, it was not detected during the first clinic conducted in Cecil County. In zip codes that contained cattle operations, the contamination of wells by total coliform bacteria was 1. Similarly, in zip codes that contained broiler, cattle, dairy, turkey, and aquaculture operations, the contamination of wells by fecal coliform bacteria was more likely than in zip codes that did not contain one of these operations; however, none of these associations were significant. The presence of broiler, hog, and turkey 61 operations in zip codes was slightly protective for total coliform bacteria, and the presence of hog operations in zip codes was slightly protective for fecal coliform bacteria (Table 3). However, these findings were not significant for any type of operation with either indicator bacterium. These findings are consistent with previous studies of private water wells that have been conducted in other states. A recent study of private wells in Pennsylvania found that 41% of wells failed to meet at least one drinking water standard (Swistock et al. Similarly, in Wisconsin, an analysis of private water wells in rural areas found that 47% of these wells exceeded one or more health-based water quality standards (Knobeloch et al. Total coliform bacteria was also the most common microbiological contaminant in the Pennsylvania study and was detected in 33% of wells (Swistock et al. A recent study of private wells in Virginia found that 46% tested positive for total coliform bacteria, with 10% testing positive for E. Meanwhile, a North Carolina study of private wells found that 49% tested positive for total coliform bacteria and 6. In our study, the county with the highest percentage of wells that tested positive for fecal indicator bacteria was Kent County, which was sampled in the Fall (Table 1). However, because our study was cross-sectional, we did not collect samples over multiple seasons and, therefore, we cannot evaluate whether seasonal trends influenced our results. Nevertheless, our study adds to the growing body of research nationwide on the water quality of private wells that illustrates the need for improved monitoring of these wells. Monitoring of fecal indicator bacteria in private well water is important for assessing the potential health risks associated with these water sources. To improve understanding of environmental factors that may impact private well water quality, we also investigated whether proximity to animal feeding operations was associated with microbial contamination of wells. Our data showed that there were no statistically significant associations between the presence of an animal feeding operation within a zip code and microbial contamination of private wells within the same zip code; however, this may be due to the small number of well water samples obtained during this initial study. Given that exposure to well water has been shown as an important risk factor for gastrointestinal illnesses (Carrique-Mas et al. The potential for private wells to influence gastrointestinal illnesses such as campylobacteriosis (that are traditionally thought to be foodborne) remains understudied in the U. One major challenge of improving private well water quality and reducing the risk of adverse health outcomes associated with this water source is that the numbers and locations of U. Neither individual counties nor states have a complete database with addresses and other contact information for private well homeowners. As such, regular communications to homeowners reminding them to test their wells annually and delivering interventions where necessary is challenging. Creating a nationwide database of 64 private well owners that is regularly updated by states could allow for improved evaluation of the factors that may influence well contamination, enhanced communication with well owners, and potential improvements in levels of waterborne illness. In this study, we demonstrated the presence of fecal indicator bacteria in private drinking water wells in Maryland. As the presence of these indicator bacteria suggests a potential human health risk, well owners are often left to mitigate these risks through system repair, enhancement, or decontamination. However, knowledge of the contamination source of the well would be helpful in selecting an appropriate remediation method. Given the small, cross-sectional nature of our study, there are several limitations to be considered. Our sample size of 118 households was relatively small, representing only a small fraction of the estimated 1,070,000 people who rely on private wells in Maryland (Maupin et al. Another limitation is the possibility that study participants may have improperly collected the water sample in their homes, which could then influence our ability to accurately determine their water quality parameters. We sought to minimize this potential problem by training participants on water sampling techniques during the safe drinking water clinic kickoff meetings, and by providing instruction sheets (along with the water sampling kits) on how participants should collect their water samples. Census of Agriculture data from 2007 with results from well water samples that were collected between 2013 and 2014. As noted above, the Census of Agriculture data were only available at the zip code level for the 2007 Census, and not for subsequent years. However, it is unlikely that the number of animal feeding operations in Maryland changed significantly between 2007 and 2013. Despite these limitations, this is the first study to assess the water quality of private wells across multiple counties in Maryland, and to investigate the influence of animal feeding operations on well water quality, thereby addressing an important research gap in the state. This study also demonstrated the value in partnerships between land grant university research faculty and county-based extension faculty. Finally, the study highlighted the need for more educational outreach to private well 66 owners in Maryland in order to improve private drinking water quality in the state. Additional studies are needed to identify and confirm potential factors that can influence private well water quality in Maryland, such as animal feeding operations, septic tanks, well construction characteristics, soil geology, and climatic conditions. This finding is similar to studies conducted in other states, including the nearby states of Virginia and Pennsylvania. In addition, while other studies have reported associations between proximity to animal feeding operations and microbial contamination of private wells, this association was not observed in this crosssectional study and may have been influenced by our limited sample size. Further studies are needed to identify and confirm possible sources of contamination of private wells in Maryland. The lack of regular monitoring of private wells makes periodic assessments at national, regional, and local scales important sources of information about this key source of drinking water throughout the U. The presence of microbial contaminants at levels greater than human health-based standards in 43.
Please tell me where the founders of Osteopathy and Chiropractic can obtain these degrees cholesterol levels too low proven 10mg rosuvastatin. All pseudo discoverers cholesterol levels keto rosuvastatin 10 mg otc, developers and founders of Chiropractic have obtained that degree from me cholesterol levels when to take medication generic rosuvastatin 10 mg amex, the Fountain Head of the science cholesterol test food before order rosuvastatin 10 mg on-line. The prominent symptoms of pleurisy are, pain in the thorax followed by a chill-the sensation produced by the involuntary contraction of the cutaneous muscles-fever and a sharp sticking pain in the side. As pleurisy advances, the patient coughs less, has less pain, lies upon the affected side, which heretofore he has not been able to do, he has less fever and his appetite may be improved. These symptoms are delusive, for we notice the breathing is more hurried, being confined to the unaffected side. Ausculation by ear or percussion on the painful side will reveal less friction and a dullness, owing to serum or pus infiltration or both. The functions of breathing and blood circulation are accelerated; digestion and the serous circulation are impeded. An undue amount of heat increases the number of red corpuscles in the blood and accelerates its action. The pleural cavity is a capillary space containing a little fluid which lubricates the opposed surfaces of the visceral and parietal membranes. Inflammation thickens and condenses the visceral covering of the lung; therefore, pus may result from the inflamed membrane, the passage of the serum may be withheld and an accumulation of serum or pus or both may fill the pleural cavity. The unusual conditions referred to are those of inflammation and fever which produce abnormal metabolism. One is a fluid searching its level, the other is impulses destined for expression. The former gains power by being obstructed, the latter will not pass an obstruction. Chiropractors are losing nothing by their advancement; the world is being benefited. Still, the founder of Osteopathy, says: "Natural flow of blood is health; and disease is the effect of local or general disturbance of blood-that to excite the nerves causes muscles to contract and compress venous flow of blood to the heart; and the bones could be used as levers to relieve pressure in nerves, veins and arteries. Still, the founder, and one of the first teachers of osteopathy, states in his masterly work on osteopathy, a book of 851 pages: "Diseases are recognized as only the result of the interruption of the onward flow of the fluids of the body, in their various rounds to build up and tear down the various tissues in itself, and that when these tissues are normally built up and the waste material properly eliminated, health is the inevitable result. A system of drugless healing by which a practitioner by a thorough knowledge of Anatomy and Physiology and by appropriate manipulation adjusts structure, so that nature can restore conditions of normal function to the body. He defines osteopathy as follows: "Osteopathy may be formally defined as the science which consists of such exact, exhaustive and verifiable knowledge of the structure and functions of the human mechanism, anatomical, physiological and psychological, including the chemistry and psycho-physics of its known elements, as has made discoverable certain organic laws and remedial resources within the body itself, by which nature under the scientific treatment peculiar to osteopathic practice, apart from all ordinary methods of extraneous, artificial, or medical stimulation, and in harmonious accord with its own mechanical principles, molecular activities and metabolic processes, may recover from misplacements, disorganization, derangements, and consequent disease and regain its normal equilibrium of form and function in health and strength. Their frequent use of drugs and surgery, and the teachings of their schools prove to the contrary. The parent school at Kirksville has a hospital where surgery is the last osteopathic manipulation. Dudley Tait, of San Francisco, makes a public statement that I think is not far from the truth. In acute poisoning, the usual medical antidotes are used-these are taught in all osteopathic schools the same as in the medical schools. In variola, they use carbolic acid or mercuric chloride solution to prevent pitting. Osteopaths occasionally write prescriptions for drugs or give verbal orders for their use, notwithstanding their claim that they are opposed to the use of drugs as remedial agents. It is stated that patients who were treated at the Philadelphia College of Osteopathy were advised to use certain medicaments at home, when osteopathic manipulations had failed to relieve. I have personally known them to advise the use of remedies that were not osteopathic, yet they state that they are oppose to the use of drugs because of their poisonous effects. Would we not be justified in believing that where diseases are treated by remedies other than osteopathic that "Osteopathy is a sort of gymnastic specialty" You be able to get away from those whom you have wronged, away from yourself, never. The spleen is situated in the left hypochondrium, below the diaphragm, above the colon, between the stomach and the cartilages of the false ribs, above and anterior to the right kidney. But they may be a considerable distance from it; they have been found embedded in the head of the pancreas. These accessory spleens are of the same structure, and vary in size from a pea to that of a walnut. The spleen is regarded by anatomists as a hematopoietic organ-one concerned in the process of blood making. After its extirpation there is an overgrowth of the lymphatic glands to compensate for its absence. Landois remarks that the spleen is a ductless gland whose activity is still, for the most part, shrouded in obscurity. In malarial and typhoid fevers this gland is found to be enlarged; sometimes from two to three times its usual size a condition usually the result of malarial poisoning and known as hypertrophy or in common language ague cake. Splenomegaly is an enlargement of the spleen; this may be of the nature of a cyst or carcinoma or both. Delafield says, sarcoma and carcinoma may occur in the spleen by extension from some adjacent part, as the stomach. A splenic cough may be recognized by being dry and unsatisfactory, no expectoration. From my observations I have been led to believe that the spleen furnishes a fluid which passes into the stomach by physiologic organic absorption, osmosis and imbibition. This splenic fluid assists digestion; it is to the stomach what bile and pancreatic juice is to the intestines. Previous to adjusting, relieving the splenic nerves of innervation, the stools were few and scanty. While adjusting the dorsal vertebra there were twenty to thirty evacuations a day, all of which, except two or three, were apparently wholly of oil; the size of the spleen being reduced accordingly. It is firmly attached to the bone by its surface, while the other is smooth, polished and free, thus reducing friction to a minimum. Hyaline cartilage was so named because the thin slices which cover the opposing surface of a joint are as hard and transparent as glass. Joints are well supplied with sensory nerves; but, neither the articular cartilage nor the articular surfaces have nerves. His twisting, deep breathing and his screaming, made the case difficult to adjust, as it was necessary to give him the thrust while slack, when the tension was off. One adjustment replaced the displaced vertebra, with a crashing sensation that could be felt and heard. The first aid to the injured had been effectual, so there was no need of transportation to the hospital. The object of language should be the expression of thot in the clearest and most attractive manner. Every writer or speaker will, of course, have a style of expression peculiar to himself, but there are some qualities essential to all good styles, namely, clearness, force and harmony. The sentence may be long and consist of many parts, but the parts should be so closely and skillfully combined as to give the impression of one symmetrical whole. The following quotations are samples of indistinctness, inharmony and lack of understanding. This experienced Chiropractor had had four months tuition in the school room and less than a month of practice when he wrote the above. A specific Chiropractor would be one specially indicated, as a sign or symptom, especially pointing out the proper course of treatment. A pure Chiropractor would be one free from mixture, in contradistinction from a mixed character or a mixture of ingredients. An unadulterated Chiropractor would be one who is free from admixture of inferior, impure, or of less valuable ingredients, for gain, deception or concealment. Heat was formerly supposed to be a subtle, imponderable fluid, to which was given the name caloric. It is now known to be a form of energy, probably the kinetic energy of confused oscillating motions of the particles of molecules of matter. Degrees of temperature represents intensities, not quantities, of heat, for when the same amount of heat is imparted to two bodies of equal mass but of different substances one is found to be hotter than the other; and we say that the specific heats of the two substances are different.
Variety: An identifiable strain within a species cholesterol lowering diet plan australia generic 10mg rosuvastatin fast delivery, usually referring to a strain which arises in nature as opposed to a cultivar which is specifically bred for particular properties; sometimes used synonymously with cultivar cholesterol examples generic rosuvastatin 10 mg. Worker: In social insects score cholesterol esc buy rosuvastatin 10mg fast delivery, a member of the sterile caste that assists the reproductive individuals cholesterol medication niaspan buy 10 mg rosuvastatin with mastercard. This m od ule is one of m any w hich m ake up a course- Certificate in Beauty Therapy. Both m en and w om en regularly go to salons to have treatm ents to their hand s and feet. A m anicure involves cutting, shaping and often painting the nails, cond itioning of the cuticles and softening the skin. In this m od ule you w il learn how to provid e hand and nail services to clients. In Unit 8 you w ill learn how to provid e services to clients and give them professional ad vice in caring for their feet and their toenails. Your professional im age includ es having w ell groom ed hand s, feet, hair and skin. Your uniform m ust also be neat and clean: this includ es accessories such as your shoes. Your posture is also im portant so you m ust practise sitting and stand ing upright. The w ay you com m unicate with clients is also a part of your professional im age. You should inquire how you could help them and agree with them on the treatm ent they w ould like. If there are reasons, in your professional opinion, that prevent you d oing the m anicure or ped icure, you m ust inform them in a courteous m anner. The learning outcom es tell you w hat you should know and be able to d o by the tim e you have finished the Unit. When you see the pen icon, you know that there is a question for you to think about and answ er. This is a self-m arked activity and you w ill find the answ ers to these at the end of each Unit. After each activity, w e give you feed back to help you und erstand the im portance of the activity. You m ust m ake sure that you have com pleted your stud y of the appropriate Units in tim e to successfully com plete assessm ents. You m ust practise frequently to build com petence with a variety of clients, with d ifferent nail conditions and nail shapes. We recom m end d oing a m inim u m of 10 treatments on hands and feet before attem pting your final assessm ent. It w ill be useful for you to keep a log of the treatm ents you d o as evid ence of your progress. In Babylonia (now called Iraq) m ore than 4000 years ago m anicure and pedicure tools m ad e of gold w ere used. Old m anuscripts describe that nail polish w as used in China, Egypt and in the Rom an Empire. They w ant their hand s, feet and nails to be treated to give them a w ell groom ed appearance. It is the same as taking care of other parts of your bod y for exam ple your hair, teeth or ears. For you to provid e professional m anicure and ped icure services to clients you have to und erstand the structure of the hand s, feet and nails. In this Unit you w ill learn about the structure of the low er arm, hand and nail. Section 1: the structure of th e low er arm and hand Section 2: the structure of the nail Section 3: N ail grow th and nail shapes Learning Outcome By the tim e you have com pleted this Unit, you should be able to: d escribe the structure of the hand and foot id entify the bones of the low er arm and hand d escribe the m uscular structure of the low er arm d escribe the structure of the nail id entify d ifferent nail shapes You should take note of these learning outcom es, as they w ill help you to assess your ow n progress as you w ork through the unit. A good und erstand ing of their structure w ill help you to give the best service to your clients and help you to be able to answ er their questions. The hand is com posed of m any d ifferent bones, m uscles, and ligam ents that allow for a large am ount of m ovem ent for hold ing and grasping objects. These bones, m uscles and ligam ents allow you to use a w id e range of tools and im plements. The hand and fingers digits another nam e for finger the fingers of the hand are called digits. These four d igits can be fold ed over the palm w hich allow s you to grasp and hold objects. Each finger, starting with the one closest to the thum b, has a com m only used nam e to distinguish it from the others: We are sure that you know the names given to the fingers. Did you w rite: ind ex finger, pointer finger, or forefinger m id d le finger ring finger little finger or pinky Look at Figure 1 to rem ind yourself w hat the d ifferent parts of the hand are called. I can feel: bones in each finger bones in the palm of m y hand bones in m y w rist phalanges bones in the fingers metacarpals bones of the p alm of the hand How many could y ou feel In the palm of your hand you should have counted 5 bones, they are called the metacarpals or palm bones. These bones fit into a shallow socket form ed by the bones of the forearm, the ulna and the radius. You find these m uscles at the und ersid e (palm sid e) of the forearm and are attached by tend ons to the bones they can m ove. The supinator m uscle in the forearm makes it possible for you to turn the forearm and hand so that the palm faces forw ard or upw ard s. It is im portant for you to know and be able to id entity som e of the m uscles as they are im portant w hen m assaging the hand. There are three types of hand m uscles that provid e us with flexibility to open and close the hand. In the d iagram below nam e the bones of the hand and arm by labelling them with the letters A to E. Abd uctor m uscle Column B Muscle Function 7 H elp to separate the fingers Allow s the tip of the thum b to touch the tip of the other fingers Draw the fingers together Straighten the w rist, hand and fingers to form a straight line H elp to bend the w rist, hand and fingers Enable you to turn your palm d ow nw ard s Enable you to turn the forearm and hand so that the palm faces forw ard or upw ard s Feedback this activity will help you check your recall of the names of the bones and muscles of the hand. If you did not get all the answers correct then you should practice again and try to memorise all the difficult words and names, including their spelling. It is a transparent plate that protects the tips of fingers, toes and the nail bed. Can you think of 3 reasons w hy it is im portant for you to know the d ifferent parts of the nail You w ill also need to know w hich parts of the nail are responsible for grow th, protection, nail shape and size. This know led ge w ould enable you to prevent d am age to the nail d uring m anicure application. Free edge Hyponychium Nail plate Nail fold Nail grooves Nail bed Lunula Matrix Cuticle Figure 6: Structure of the nail keratin a p rotein w hich is the chief com p onent of the hair and nails Nail plate: the nail plate consists of keratin and semi- translucent cells packed closely together. Nail groove N ail groove are slits or tracks at either sid e of the nail upon w hich the nail m oves as it grow s. Cuticles becom e d ry from excessive exposure to w ater and chem icals and also because of the natural aging process. A m anicurist/ ped icurist pays particular attention to cuticles ensuring that they are w ell conditioned. Nail wall the nail w all is m ad e up of fold s of skin overlapping the sid es of the nail, provid ing protection for the nail. It contains nerves, lym ph, and the blood vessels that nourish the nail; it prod uces cells that generate and harden the nail. In the d iagram below label the diagram by placing the term s next to the appropriate part of the nail: free ed ge, m atrix, cuticle, lunula, nail groove, nail plate, nail w all and nail bed.
The red lines indicate perimortem fractures and the hash marks (either blue or purple ink) indicate missing bone cholesterol levels japan 10mg rosuvastatin with mastercard. Due to the use of mean ages-at-death cholesterol in peanut butter order 10mg rosuvastatin with amex, there are no individuals in the 31-35 year category cholesterol medication grapefruit juice cheap rosuvastatin 10mg free shipping. Sex ratios (for age categories with sufficient samples for ratios) for Choeung Ek crania ldl cholesterol foods avoid generic rosuvastatin 10mg line. The four bars on the left represent the 179 crania with discernable impacts, plus the 132 crania with indeterminate impact sites. Frequencies of discernable impacts by trauma mechanism (crania = 179; impacts = 198). Graph truncated to better illustrate lower frequencies of non-male, non-blunt force combinations. Graph truncated to better illustrate lower frequencies of non-male, non-blunt force combinations. Joint bi-plot derived from the contingency table data (Table 13) showing distribution of age and sex cohorts (columns) and mechanisms of trauma (rows). Money is placed into the memorial by visitors (numerous international currencies) as seen in the bottom left image. The bottom image shows traditional urns (with cremains) that have been placed in the lower half of the memorial. Around the base of the memorial are two levels of concrete-sculpted panels depicting the history of the Khmer Rouge regime in Battambang. Permission was needed to open the metal door (in the middle image) to really see the remains. The u-shaped items surrounding the bones (middle image) are leg shackles that were found in/near the graves. The remains are in the red oval in the top image; they are surrounded by trash and graffiti. The remains in good condition had been sent to another memorial at Phnom Oudong in Kamong Speu Province. The red arrow points to a pile of postcranial elements; the red oval indicates the crania distinctly set apart from the remainder of the bones (images courtesy of the Tuol Sleng Genocide Museum). Within the grounds of a single Buddhist wat there are different displays of ethnicity after death. On either side are traditional Khmer chedey, which presumably contain the urn(s) of cremated individual(s). Penetrating sharp force trauma at Choeung Ek: A) penetrating incised wound with plastic deformation on the medial edge; B) sharp force with irregular edges and radiating fracture; C) sharp force removal of anterior aspect of right temporal arch. Notice radiating fractures of lateral and basilar portions of occipital and across the palate. Transverse perimortem fracture of anterior basilar portion of the occipital associated with trauma to squamosal portion. Transverse linear fractures of the basilar portion of the occipital at the sphenooccipital suture/synchondrosis. Crania without discernable impact sites, but with missing aspects of the lateral and basilar portions of the occipital. Crania without discernable impact sites, with radiating fractures (highlighted in red) surrounding the foramen magnum, but no missing bone. In the image on the left, note the transverse fracture of the basilar portion and the radiating fracture within the left mandibular fossa. The age heaping in B is resulting in the overrepresentation of certain ages, particularly those that end in 0 or 5; the black arrows indicate the age heaping at ages 20, 25, 30, 45, 55, and 60 years. Probability density functions for the 97 Tuol Sleng execution lists and Alameda-Stone cemetery osteological data. In the center of the painting is a Khmer Rouge cadre ready to strike a bound and blindfolded victim with a farming hoe at the edge of a mass grave. To the left of the center cadre is a cadre "catching" an infant on his bayonet (another oft cited method of executing infants). The likelihood that all of these forms of violence occurred at this one site is dubious; rather, this is likely a representation of collected memories of Khmer Rouge violence. The glare makes it slightly challenging to see, but the Khmer Rouge cadre on the left is standing above three bound and kneeling victims ready to strike them with a long object, likely an iron cart axle. The artist depicts a Khmer Rouge cadre striking a kneeling victim on the back of the head with a farming hoe. A) the slightly non-circular entrance seen ectocranially; B) internal beveling on the endocranial surface. Map of bones that used to be displayed at Tuol Sleng (image courtesy of the Tuol Sleng Genocide Museum). The small plaques at the top of each stand provide brief descriptions of each cranium. Who are these men, women, and children, and what befell them during the Khmer Rouge period While their individual identities may forever be lost, the primary objective of this research is to augment knowledge and answer questions not yet addressed regarding Khmer Rouge violence in Cambodia. By systematically analyzing the human skeletal remains at the Choeung Ek Genocidal Center, which directly retain evidence of violent actions, I integrate previously undocumented data into a more holistic narrative of Khmer Rouge atrocities. This research employs a biocultural anthropological approach to address questions concerning the individuals executed by the Khmer Rouge and the agency (the effect on living individuals) of the resulting skeletal remains. To achieve this objective I analyzed hundreds of human crania at the Choeung Ek Genocidal Center to assess demographics and osteological manifestations of violence, analyzed original Khmer Rouge documents at the Tuol Sleng Genocide Museum (the former S-21 security center), and assessed the sociocultural implications of incorporating unidentified human remains into national and local memorials. It is anticipated that this research will greatly contribute to the literature on Khmer Rouge violence, as well as to the ongoing forensic anthropological focus on crimes against humanity and genocide. Only a small number of individuals, primarily Khmer Rouge officials and factory workers, were left in the cities (Ea 2005). The living conditions under the Khmer Rouge were severe, with historical estimates stating that between 1975 and 1979 approximately one quarter of the Cambodian population of nearly eight million died from mistreatment, overwork, malnutrition, and violence (Kiernan 2008). Various scholars have provided different estimates for the percentage of this figure that were executed; ranging between 30 and 40% of deaths, the number of executed individuals equates to roughly 527,000 to 680,000 (Ea 2005). In addition to establishing policies idealizing the peasantry and creating a complete agrarian economy, the Khmer Rouge sought the complete destruction of internal and external "enemies," both real and imagined. In order to suppress these enemies, security centers were established to imprison, interrogate, torture, and often execute enemies and their families (Ea 2005). On January 7, 1979 the Vietnamese army, with assistance from Cambodian supporters, overthrew the Khmer Rouge in Phnom Penh ending the three years, eight months, and 20 days of Democratic Kampuchea. The terms "genocide" and "crimes against humanity," although often used synonymously to denote violence on a large scale, have specific legal definitions. Developed in the context of the Nuremberg Trial of Nazi war crimes in the late 1940s, "crimes against humanity" is a broad category encompassing extermination, persecution, and deportation of religious, political, and racial groups (Adelman et al. The term "genocide"-derived from the Greek words genos meaning race or tribe and cide, to kill (Rothenberg 2005)-coined by Raphael Lemkin and adopted by the newly formed United Nations in 1948, is defined as "acts committed with intent to destroy, in whole or in part, a national, ethnical, racial or religious group" (Gellately and Kiernan 2003). Thus, genocide is considered the most egregious, or "aggravated," form of crimes against humanity. Additionally, crimes against humanity can only occur during times of war while genocide can be committed during both war and peace (Adelman et al. But why have 5 anthropologists and other social scientists neglected to engage themselves in research on this topic, despite being involved in research on warfare, conflict, and violence in early human societies (Hinton 2002a; Hinton 2002b) Hinton (2002a) suggests that cultural relativism, a focus on globalization, and general feelings of discomfort or insufficiency in the face of such a broad and complex topic are a few reasons anthropologists may not have actively engaged in the study of genocide. Anthropologists, as Hinton (2002b) notes, have local, sociocultural knowledge that can be directly linked to the macro-level dimensions of genocidal actions. Ethnographically, anthropologists can question the historical representations of genocides and the role of the nation-state in the formation of national identity as well as a focus on individuals and groups such as refugees in post-conflict diasporic contexts. In other words, anthropologists are able to contribute unique cultural and social information to the understanding of genocides which might otherwise be overlooked.
Correspondence analysis relies on three concepts of contingency tables-chi-square distances cholesterol ratio total hdl cheap 10mg rosuvastatin with visa, profiles cholesterol levels standard generic rosuvastatin 10 mg with visa, and masses-to generate points in space (Hefner 2007) cholesterol norms cheap rosuvastatin 10mg without a prescription. The relative distances between the points on the resulting plots provide information about the correspondence between the variables (Alberti 2013) cholesterol treatment guidelines purchase 10mg rosuvastatin free shipping. While the distances between the points are not statistically significant, if variables are found to be relatively close together on the plot, the relationships or correspondences can be further evaluated to determine if the variables are in fact associated (Monslave and Hefner 2016). A singular value decomposition performed on the standardized residuals matrix was used to plot data in two dimensions (Monslave and Hefner 2016). Again, for the sake of brevity, this statistical test will not be discussed in each individual section below. Trauma Mechanism and Fracture Type the mechanisms of traumatic injuries-blunt force, sharp force, high velocity projectile, and indeterminate mechanism-were evaluated on multiple levels. First, the frequencies of each mechanism were generated for the crania with discernable impact sites. Second, the frequencies of an individual having one mechanism of trauma, or multiple/mixed mechanisms, were 108 calculated. There were five categories of fracture types: depressed fractures, radiating fractures, concentric fractures, other fractures, and multiple types of fractures. The "other" variable was generally associated with sharp force trauma which does not often leave a fracture (it is usually an incised wound), or fractures that were indeterminate in nature. There were five multi-fracture type combinations: 1) depressed and radiating; 2) radiating and concentric; 3) radiating, concentric, and other; 4) radiating and other; and 5) depressed and other. These combinations were present on crania that only had one impact as well as those that had multiple impacts. Trauma Location As discussed in the previous chapter, for the purposes of data analysis, the cranium was divided into five regions: vault (frontal and parietal bones), basicranium (occipital, inferior sphenoid, petrous portion of the temporals), right and left lateral (temporal bones and greater wings of the sphenoid), and face (bones of the face excluding the frontal and mandible). This provided for a more efficient evaluation compared to assessing the frequency of trauma or impacts to each individual cranial bone. Another challenge that had to be addressed to effectively asses the frequencies of traumatic injuries was accounting for impacts that spanned multiple bones and/or cranial regions. Twenty-four multi-bone combinations were present for 109 perimortem impacts-two additional multi-bone combinations were identified for antemortem only trauma. While slightly reduced when bones were lumped into cranial regions, there were still 13 multi-region combinations for perimortem impacts (see Appendix). The basilar portion of the occipital bone is located between the foramen magnum and the articulation with the body of the sphenoid. In juveniles, this articulation is called the spheno-occipital synchondrosis or suture. This synchondrosis ossifies during adolescence resulting in a fusion of the occipital and sphenoid. Throughout the analytical phase, I set aside 50 crania that I reassessed between seven and 60 days after the original evaluation. The closer the resulting value is to one the higher the agreement and 110 the lower the error. The minimum, mean, and maximum ages-at-death for the entire sample were also calculated. As with the osteological data from Choeung Ek, sex ratios by age category were calculated to compare the difference in the demographic patterns between adult males and females and specific age categories (Heilen et al. Hazard models were also computed to assess the mortality and survivorship differences between males and females. Comparison of Osteological and Archival Demographics To compare the demographics between the known (archival) data, and those generated from the osteological remains at Choeung Ek, hazard modeling was used. Drawn from paleodemographic research, hazard models were applied to assess survivorship, mortality rates, and age-at-death and sex distributions. Moving away from the construction of life tables with their numerous flaws (Wood et al. Hazard models do not necessarily overcome the challenges of accurately representing an osteological sample, such as nonstationarity in a population, selective mortality, hidden heterogeneity in risk, underrepresentation of certain age groups, and the ability to accurately estimate age-at-death for older adults (Trask 2012; Wood et al. However, understanding and visualizing the demographic patterns of populations can provide important information. Survivorship refers to the probability that an individual within a population will survive to a given age (Chamberlain 2006). The probability of surviving beyond a given age is expressed as a value between 1. Conversely, mortality is the probability of a segment of the population that will die (hazard) within a given age interval (Chamberlain 2006). While mortality varies across the lifespan, and under various environmental and cultural conditions, the typical mortality model for past human populations demonstrates high juvenile mortality that decreases after approximately ten years old and remains fairly constant (low) for adolescents into early adulthood. With older age there is again a rise in mortality (Chamberlain 2006; Ubelaker 1989). For this research, a Siler hazard model was used to evaluate the associations between the osteological data from Choeung Ek and the archival execution list data from Tuol Sleng. The Siler model, unlike the Gompertz model, incorporates the subadult age categories to assess the full lifespan (Wood et al. The Siler model builds on the Gompertz model-which describes the age-independent (adulthood, typically accidental or deaths due to childbearing) and 112 senescent (older adulthood) hazards-by adding and describing a juvenile (subadulthood) hazard component. For this research, a four-parameter Siler function was utilized to evaluate survivorship and mortality across the entire lifespan. The four parameters are represented by 1 and 1 (the juvenile component) and 3 and 3 (the senescent component). The 2 parameter (the age-independent component) is excluded from this Siler function, according to Herrmann and Konigsberg (2002), because it is difficult to reliably estimate in paleodemographic samples due to heterogeneity in risk of mortality (Wood et al. In order to utilize the Siler hazard model, sample age-at-death distributions were required. The archival and osteological data were therefore distributed into age-at-death categories as follows: 0-1 year, 2-5 years, 6-10 years, 11-15 years, 16-20 years, 21-25 years, 2630 years, 31-35 years, 36-40 years, 41-50 years, etc. For the archival data, age-at-death greater than 50 years continued to be divided into 5-year brackets. For the osteological data, age-atdeath greater than 50 years was defined as one bracket. In general, five-year age categories were used because, according to Ubelaker (1989), five years is long enough to encompass probable errors in the age estimate and short enough to permit the recognition of patterns across the sample. For the archival data, this process was straightforward as nearly all individuals on the execution lists had an age (point estimate) documented. For those that did not have an age recorded, the mean age-at-death for the archival sample (29 years) was assigned. The osteological data required more manipulation as anthropological assessments of age-at-death do not result in point age estimates. During data collection at Choeung Ek, as discussed in the prior chapter, I initially assigned each individual to a narrow age category based on dental 113 development and/or maxillary and cranial suture closure. The means of these narrow age categories were used as the point age estimates for the hazard model data. The mean point age estimates for the juveniles were: fetal, 1, 4, 7, 10, 13, and 16 years. At the time of data collection, two individuals had only been assigned to broad age categories. One individual was determined to be a young adult and the one was an adolescent; the mean ages of these broad categories were thus used for these individuals (27. After these age-at-death frequency distributions were created for the total osteological and archival samples, the frequencies were distributed by sex. However, because sex cannot be estimated for juvenile and adolescent skeletal remains, all individuals younger than 20 years old were removed from both the archival and osteological data when the samples were divided by sex. Again, for the archival data, dividing the sample by sex was straightforward as sex and age were documented. Individuals without their sex recorded were removed from the sample, and again, individuals without a designated age were assigned the sample mean of 29 years. First, the original categories assigned for sex (male, probable male, female, or probable female) needed to be combined. Probable males were pooled with males and probable females were pooled with females. The resulting probability density function and survivorship and mortality graphs permitted comparisons of survivorship and mortality distributions between the total samples and between the sexes for the osteological and 114 archival data.
Order 10 mg rosuvastatin visa. Savage on Health - Exposing the Cholesterol Myth - The Truth about HDL LDL & LPA Levels.