X



|
STUDENT DIGITAL NEWSLETTER ALAGAPPA INSTITUTIONS |

|
"Buy desloratadine 5 mg without a prescription, allergy medicine voice".
X. Yespas, M.B.A., M.D.
Professor, University of North Texas Health Science Center Texas College of Osteopathic Medicine
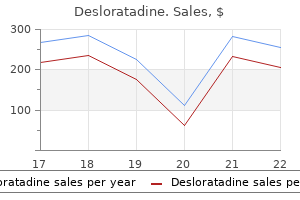
The final common pathway in virtually every instance is a cellular genetic mutation that converts a well-behaved cellular citizen of the body into a destructive renegade that is unresponsive to the ordinary checks and balances of a normal community of cells allergy shots problems 5mg desloratadine mastercard. Promoters (oncogenes) and suppressors (like the retinoblastoma or p53 gene) play a central role in many cases (see Chapter 191) allergy symptoms on kids order desloratadine 5 mg otc. Chemicals such as benzene and nitrosamines allergy testing list purchase desloratadine 5mg online, physical agents such as gamma and ultraviolet radiation allergy report nj buy desloratadine 5 mg on-line, and biologic agents such as the Epstein-Barr and hepatitis viruses contribute to carcinogenesis under certain circumstances. Evidence exists to link dietary factors to carcinogenesis; although not as clear as one would like, the evidence is strong enough to recommend diets low in fat and high in fiber. A sensible diet is based on grains, vegetables, and fruits, with smaller than the current average proportions of fat. Inherited susceptibilities are becoming more evident and probably play a key role in a significant number of cancers of the breast and colon. Down syndrome and the Li-Fraumeni syndrome are well-known harbingers of a substantial risk for developing cancer. The single most important carcinogen in the United States and Europe is tobacco (see Chapter 13), because it causes or contributes to the development of about one third of all cancers: primarily lung, esophageal, head and neck, and bladder. Less well appreciated is the contribution tobacco may make to causing breast, colon, and gastric cancer. Tobacco-related cancer is also important because it is preventable by the obvious, inexpensive, and 100% effective means of abstention. Although the total number of smokers in the United States has declined, women smoke more than ever, adolescents continue to view smoking as socially chic, and the number of smokers in Asia and developing countries is growing at an alarming rate. When prevention of cancer is not possible because effective means are lacking, early detection is the next best strategy to reduce cancer mortality. As a general rule, the smaller and more confined the tumor, the more likely therapy will result in permanent cure. This approach has been most successful for directly accessible tumors that have an early malignant or premalignant state. Examples include Papanicolaou smears and surgical conization for cancer of the uterine cervix, physical removal of early skin cancer, and colonoscopic removal of colorectal polyps. However, it is not clear that all in situ breast and prostate cancers will become invasive and fatal, so there is some risk of overtreatment, particularly for prostate cancer. An even more exciting development in this effort has been the emergence of genetic screening and counseling of families at high risk for developing cancer. Individuals at risk are identified largely by analysis of family pedigrees, and the increasing availability of the revolutionary tools of molecular biology can identify specific genetic mutations (see Chapter 191). It is certain that many such genes will be identified, focusing the cancer screening and early detection efforts more efficiently and productively on high-risk populations (see Chapter 190). Although it is impossible to know the specific details of early in vivo tumor growth and the efficiency of tumor cell renewal of human cancer, clinical and laboratory observations have provided a reasonable conceptual framework. This framework should be used with caution, however, because it is certain that the intrinsic factors that control tumor growth and propagation are far more complex, episodic, and heterogeneous than currently known, even within a single tumor mass. Furthermore, the stromal environment and neovascularization of tumors have become more central to our understanding of this process than heretofore. A tumor reaches the size of clinical detectability when it contains about 109 cells, weighing about 1 g and occupying a volume of about 1 mL. Below 109 cells, the tumor is usually undetectable, but it has already undergone at least 30 doublings, and only 10 further doublings will produce the 1 kg of tumor. This exercise illustrates how much has already occurred, with all the opportunities for the cancer to undergo advantageous mutation and metastasis, before clinical detection. Once the tumor has grown into the clinically evident range, it tends to grow progressively slower with increasing size. This deceleration of growth probably occurs because the tumor outgrows its blood supply, reaches anatomic Figure 189-1 A schematic representation of the phases of growth of a cancer. After a period of inapparency (lag phase), growth tends to be logarithmic, followed by deceleration due to inadequate nutrients, competitive inhibition among cells, or a lack of neovascularization. Thus, cancers probably grow much like bacteria after inoculation into a favorable medium.
Contaminated reusable equipment should be decontaminated using heat sterilization allergy nose best 5 mg desloratadine, or when heat is impractical allergy symptoms coughing at night desloratadine 5mg without prescription, using a mycobactericidal cleanser allergy shots make you tired order desloratadine 5mg. Pocket masks or mechanical ventilation devices should be available in areas where cardiopulmonary resuscitation procedures are likely allergy testing babies desloratadine 5mg with amex. Health care workers with open lesions or weeping dermatitis should avoid direct patient contact and should not handle contaminated equipment. Private rooms are not required for routine care; select circumstances, however, such as the presence of concomitant transmissible opportunistic disease, may warrant respiratory, enteric, or contact isolation. Health care workers with denuded skin, open lesions, or active dermatitis should avoid direct patient contact and should not process contaminated equipment or materials. Because all blood and body fluids should be handled as potentially hazardous and all patients presumed to be infected, it makes little sense to identify infected patients or their specimens with "blood and body fluid" labels. The use of such labels on known infected patients implies that unlabeled specimens or specimens from patients of unknown status are less hazardous and may be handled with less care. Although sharp injuries cannot be entirely eliminated, the number of exposures can be reduced substantially by adhering to guidelines put forth in universal precautions. Before a sharp instrument is used, thought should be given regarding where the instrument will be disposed after use. Impervious containers should be readily available in all patient care areas and identified by the health care worker prior to "sharp" utilization. The containers should be checked frequently and should not be allowed to overfill. Recapping of needles is the single most common activity that results in needle stick injuries. Despite their logical basis and relative ease of implementation, universal precautions have not been used routinely by many health care providers. Although lack of adequate education may partly explain these findings, implementation of infection control practices has been generally poor historically. Between 200 and 400 health care workers die each year as a result of hepatitis B infection acquired on the job. The essential elements of management following needle stick or mucous membrane exposure include defining the type of exposure, appropriately evaluating the donor (patient) and recipient (health care worker) at the time of exposure, and follow-up of the health care worker for at least 1 year after exposure. If the patient refuses or cannot give consent, he/she should be considered to be infected. The health care worker should report any acute illnesses that occur during the follow-up period, especially during the first 6 to 12 weeks after exposure. Serologic testing should be made available to all health care workers who are concerned about potential on the job exposure. Body fluids considered to be potentially infectious include blood, blood products, cerebrospinal fluid, amniotic fluid, menstrual discharge, inflammatory exudates, pleural fluid, peritoneal fluid, pericardial fluid, and any fluid visibly contaminated with blood. Recommended Recommended Available Discouraged 1907 who experience a massive or definite parenteral exposure. Many clinicians favor using prophylactic antiretroviral therapy after possible parenteral exposures, although this practice remains controversial. The firm recommendation to administer routine chemoprophylaxis in cases of massive or definite exposure is based on increasing evidence of the beneficial protective effects from its use in both animal and human studies. Therefore, in most medical centers, multidrug chemoprophylaxis has become a standard of practice. Health care workers with doubtful parenteral or nonparenteral exposures generally should not take chemoprophylaxis. The optimal timing and dosage of chemoprophylaxis are unknown; however, animal studies suggest that higher doses given as soon as possible after exposure have the best chance of being effective. Therefore, most centers that offer chemoprophylaxis to their employees have established mechanisms whereby the health care worker can be evaluated and the drugs administered within 2 to 4 hours after the exposure. Six patients are believed to have acquired infection from the dentist based on the absence of other risk factors among the patients and the high degree of homology between the viruses isolated from the dentist and those isolated from the patients. Although each patient underwent an invasive procedure in the dental office, the precise mode of transmission remains unknown.
As the pathways for lateral eye movements (the pontine gaze center allergy testing routes purchase desloratadine 5mg mastercard, medial longitudinal fasciculus allergy treatment plano buy desloratadine 5mg without a prescription, and oculomotor-third nerve-nucleus) traverse the reticular activating system allergy testing codes proven desloratadine 5mg, impairment of reflex eye movements is often the critical element in diagnosis allergy medicine 3 month old baby desloratadine 5 mg. A comatose patient without impairment of reflex lateral eye movements does not have a mass lesion compromising brain stem structures in the posterior fossa. Posterior fossa lesions may compromise cortical function by upward herniation across the cerebellar tentorium or by blocking of cerebral spinal fluid flow from the lateral ventricles, resulting in the dangerous state of non-communicating hydrocephalus. Metabolic abnormalities characterize syndromes caused by the presence of exogenous toxins (drugs) or endogenous toxins (organ system failure), resulting in diffuse dysfunction of the nervous system without localized signs such as hemiparesis or unilateral pupillary dilatation. A diagnosis of "metabolic encephalopathy" indicates that the examiner has found no focal anatomic features in examination or neuroimaging study results to explain coma but does not state that a specific metabolic cause, such as hypernatremia, has been established. Drugs have a predilection for affecting the reticular formation in the brain stem and producing paralysis of reflex eye movement on examination. Generalized seizures produce diffuse abnormal electrical discharges throughout the reticular formation and cortex, thus satisfying the anatomic criteria for coma. In the late stages of status epilepticus motor movements may be subtle even though seizure activity is continuing throughout the brain. Once seizures stop, the abnormal electrical activity is followed by a state of electrical inhibition, which may be prolonged. This so-called post-ictal state produces coma and if the inciting seizures are not witnessed can also be a cause of unexplained coma. A premonitory headache supports a diagnosis of meningitis, encephalitis, or intracerebral or subarachnoid hemorrhage. A preceding period of confusion or delirium points to a diffuse process such as meningitis or effects of endogenous or exogenous toxins. The sudden apoplectic onset of coma is particularly suggestive of ischemic or hemorrhagic stroke affecting the brain stem or of subarachnoid hemorrhage or intracerebral hemorrhage with intraventricular rupture. Lateralized symptoms of hemiparesis or aphasia prior to coma occur with hemispheric masses. Coma associated with cholinergic signs: lacrimation, salivation, bronchorrhea, and hyperthermia. Although not invariably present and having varying sensitivity in regard to cause (very common with acute pyogenic meningitis and subarachnoid hemorrhage, less common with indolent, fungal meningitis), the presence of signs of meningeal irritation on examination is the central clue to the diagnosis. Passive neck flexion should be carried out in all comatose patients unless head trauma is likely to have occurred. When the neck is passively flexed, attempting to bring the chin within a few finger-breadths of the chest, patients with irritated meninges will reflexively flex one or both knees. In the absence of lateralized signs (such as hemiparesis) indicating a superimposed mass lesion, a spinal puncture should be performed immediately. Although rare cases of herniation after lumbar puncture in children with bacterial meningitis have been reported, the urgency of diagnosis and treatment at the point of coma is paramount. Structural and metabolic causes of coma can be distinguished by neurologic examination: As the evaluation and potential treatment modalities for structural versus metabolic coma are widely divergent and the disease processes in both are often rapidly progressive, initiating the evaluation in a medical or surgical direction may be life-saving. This task is accomplished by focusing on three features of neurologic examination: the motor response to a painful stimulus, pupillary function, and reflex eye movements. The functioning of the motor system provides the clearest indication of a mass lesion. Elicitation of a motor response requires that a painful stimulus to which the patient will react be applied. The arms should be placed in a semiflexed posture and a painful stimulus applied to the head or trunk. Strong pressure on the supraorbital ridge or pinching of skin on the anterior chest or inner arm is most useful; nail bed pressure makes the interpretation of upper limb movement difficult. The evolution of neurologic signs from an expanding hemispheric mass lesion is illustrated in Figure 444-1 (Figure Not Available). This lateralized motor movement in a comatose patient establishes the working diagnosis of a hemispheric mass. As the mass expands to involve the thalamus (late diencephalic) the response to pain is now reflex arm flexion associated with extension and internal rotation of the legs (decorticate posturing); asymmetry of the response in the upper extremities will be seen.
The increase 1167 in proteolysis is primarily caused by the actions of hormones and cytokines allergy symptoms on the lips purchase desloratadine 5mg line, with additional protein losses occurring in specific disease states allergy gainesville band desloratadine 5mg with amex. In general allergy spray buy 5mg desloratadine, hospitalized patients with normal renal and hepatic function should receive 1 allergy medicine green box buy cheap desloratadine 5mg online. For the majority of patients, provision of greater amounts of protein does not provide benefit, and the excess protein results in ureagenesis. For obese patients (weight greater than 120% of ideal weight), it may be appropriate to provide 1. The administration of nutrition support to critically ill, immobilized patients can decrease but not prevent the loss of body protein. Modified amino acid solutions have been formulated for use in specific disease states. For example, the use of branched-chain enriched amino acid solutions (providing up to 50% of amino acids as leucine, isoleucine, and valine) has been suggested for patients with hepatic encephalopathy. These patients have decreased plasma levels of branched-chain amino acids and increased levels of aromatic amino acids. Branched-chain amino acids are uniquely oxidized in skeletal muscle and adipose tissue rather than the liver. Several studies indicate that patients prone to encephalopathy can tolerate more protein being given as branched-chain enriched solutions than as the standard solution. However, the clinical effectiveness of formulas with high levels of branched-chain amino acids is controversial inasmuch as few prospective randomized trials have compared this treatment with standard therapy. Once the encephalopathy has resolved, the less costly standard amino acid solution should be used. Patients with liver disease but no encephalopathy can tolerate the less costly standard amino acid solutions. Limited data support the use of branched-chain amino acid solutions for patients with renal failure or severe stress. Another example of a modified amino acid formulation is a more concentrated (15%) amino acid base solution. Use of this product enables higher caloric and protein supplementation in less volume to patients with excess total body water and salt. The disadvantages of this product are similar to those of branched-chain solutions: its expense and the lack of prospective, randomized trials confirming its efficacy. Parenteral nutrition supplementation with the amino acid glutamine is undergoing investigation. Currently, glutamine is not present in commercially available parenteral nutrition solutions in the United States because it has a shorter shelf life than the more commonly used amino acids and has been considered a non-essential amino acid. During critical illness, however, glutamine appears to be an essential amino acid for the intestinal tract. For patients undergoing bone marrow transplantation, the use of glutamine-supplemented parenteral nutrition (as compared with the standard amino acid solution) has been shown to improve clinical outcome with fewer infections and shortened hospital stay. Parenteral carbohydrate provided in the form of dextrose is a vital source of fuel and has important nitrogen-sparing effects. Solutions of dextrose in concentrations of 10 to 70% are mixed with the appropriate quantity of amino acids to obtain the desired solution. The minimum daily glucose requirement is the amount necessary to meet brain glucose needs (100 to 150 g) because body carbohydrate stores are limited. Providing calories as glucose stimulates insulin secretion, reduces muscle protein breakdown, and decreases hepatic glucose release, thus decreasing the need for skeletal muscle to provide amino acid precursors for gluconeogenesis. Fat emulsions provide an intravenous source of fat calories and the essential linoleic and linolenic fatty acids. The emulsions contain long-chain fatty acids (derived from safflower and/or soybean oil), egg yolk phospholipids as emulsifying agents, and glycerin to make the solution isotonic with plasma. Intravenous fat is calorically dense (9 kcal/g), isotonic, and protein sparing and can prevent essential fatty acid deficiency. In addition, provision of a portion of calories as fat allows lower rates of dextrose infusion, which results in less hyperglycemia and hyperinsulinemia and a lower incidence of abnormalities in liver function tests.
Although estrogen use appears to be protective allergy medicine 9 month old generic desloratadine 5 mg with amex, the magnitude of its effect must ultimately be determined in prospective allergy medicine overdose symptoms desloratadine 5mg on line, randomized clinical trials allergy medicine for ragweed order desloratadine 5mg without prescription. This range is wide allergy shots dangerous generic desloratadine 5 mg amex, and any small change in relative risk results in a great reduction in mortality. The cardiovasclar effect of estrogen is partially due to an improvement in lipids and lipoproteins (30-40%), with the remaining effect due to vascular changes, insulin sensitivity, and so on, as described above previously. For cardiovascular disease mortality, a protective effect 10-fold greater than that for osteoporosis is estimated. The annual economic benefit on cardiovascular disease is estimated at $60 billion, and that for osteoporosis is $10 billion. Ischemic heart disease, osteoporotic fractures, breast cancer, and endometrial cancer are four events that are potentially affected by estrogen use. The case-fatality rate for ischemic heart disease is greater than that for osteoporotic fractures and both types of cancer combined. Although the magnitude of the association between estrogen and endometrial cancer is controversial, these figures reflect a relative risk of only 2. Another controversial issue is the risk of breast cancer with estrogen use, if we assume, a risk of 1. Clearly, the change in mortality with estrogen use is greatest for ischemic heart disease. In calculating the cumulative change in mortality, approximately 41% of women benefited by taking estrogen. Although these were calculated data, these findings have been corroborated in several cohort studies. Each has demonstrated an overall 40% reduction in all-cause mortality with estrogen. Two studies have shown that the benefit in mortality is related to the duration of use; but one has suggested that the effect is decreased beyond 10 years of use because of an increase in breast cancer mortality that was present in this cohort (nurses). These data are not consistent with these reports, which have shown either no change in breast cancer mortality with estrogen use or actually a decrease in mortality. Mortality from stroke has also been shown to decrease by approximately 40% with estrogen use. However, the literature is less consistent about stroke than the effect on ischemic heart disease. In general, the data are consistent in showing decreased mortality and an increased longevity (1 to 2. The benefit is greatest for those with cardiovascular risk factors and is least for those with significant risk factors for breast cancer. Endometrial disease occurs with unopposed estrogen therapy in women who have a uterus. Thus, the risk is far less for endometrial cancer than it is for varying degrees of hyperplasia. One recently conducted study showed that the risk of endometrial hyperplasia was 20% after 1 year of use of 0. In another study, the 3-year postmenopausal Estrogen/Progestin Interventions Trial, this risk was approximately 40% at the end of 3 years. No cancers were reported in either of these two studies, and the addition of a progestin essentially eliminated the hyperplasia. The risk of developing endometrial cancer is the same for a woman taking estrogen and progestin (hormone replacement therapy) as for the general population. The addition of a progestin merely eliminates the excess risk induced by estrogen. Other endometrial cancers occurring in postmenopausal women are not thought to be hormonally related. Although the risk of developing endometrial cancer is increased significantly in estrogen users, the risk of death from this type of endometrial cancer does not increase proportionately. Endometrial cancers associated with estrogen use are thought not to be as aggressive as spontaneously occurring cancers or that tumors in women taking estrogen are likely to be discovered and treated at an earlier stage, thus improving survival rates.