X



|
STUDENT DIGITAL NEWSLETTER ALAGAPPA INSTITUTIONS |

|
"Buy cheap hydrochlorothiazide 25 mg, blood pressure below 60".
T. Samuel, M.A., M.D., Ph.D.
Clinical Director, Cleveland Clinic Lerner College of Medicine
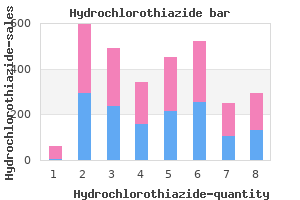
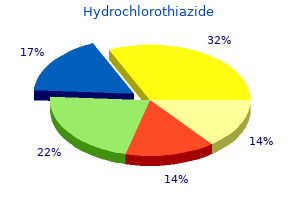
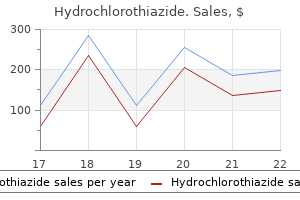
For youth arrhythmia treatments hydrochlorothiazide 25 mg with amex, regular physical activity can improve bone health pre hypertension emedicine discount hydrochlorothiazide 25mg mastercard, cardiorespiratory and muscular fitness primary pulmonary hypertension xray 12.5mg hydrochlorothiazide mastercard, and cognition (including academic achievement) hypertension uncontrolled generic 12.5 mg hydrochlorothiazide visa, and reduce the symptoms of depression. Preschool-aged children should be active throughout the day to enhance growth and development. Adults caring for children during this age should encourage active play that includes a variety of activity types (light, moderate, or vigorous intensity) and aim for at least 3 hours per day. School-aged children and adolescents need at least 60 minutes of moderateto-vigorous activity daily to attain the most health benefits from physical activity. Most activity can be aerobic, like walking, running, or anything that makes their heart beat faster. They also need muscle-strengthening and bone-strengthening activities that make their muscles and bones strong, like climbing on playground equipment, playing basketball, and jumping rope. Nutrient-Dense Foods and Beverages Nutrient-dense foods and beverages provide vitamins, minerals, and other healthpromoting components and have little added sugars, saturated fat, and sodium. Vegetables, fruits, whole grains, seafood, eggs, beans, peas, and lentils, unsalted nuts and seeds, fat-free and low-fat dairy products, and lean meats and poultry-when prepared with no or little added sugars, saturated fat, and sodium-are nutrientdense foods. Figures 3-1, 3-3, 3-5, and 3-7 display the average intakes of the food groups compared to the range of recommended intakes at the calorie levels most relevant to males and females in these age groups. Additionally, the percent of children and adolescents exceeding the recommended limits for added sugars, saturated fat, and sodium are shown, along with average intakes of these components. Average intakes compared to recommended intake ranges of the subgroups for grains are represented in daily amounts; subgroups for vegetables and protein foods are represented in weekly amounts (see Figures 3-2, 3-4, 3-6, and 3-8). Current intakes show that from an early age, dietary patterns are not aligned with the Dietary Guidelines. The Healthy Eating Index score of 61 out of 100 for children ages 2 through 4 indicates that overall diet quality is poor. Among children ages 2 through 4, consumption of total fruit is generally adequate for about 60 percent of children. Compared to other age groups, a higher percentage of young children also have intakes of total vegetables at or above recommended levels. The difference between recommended and actual intakes of total fruit and total vegetables emerges and expands as children age. By late adolescence, average fruit and vegetable consumption is about half of the recommended range of intake. For fruit, about 70 percent of intake comes from whole forms-fresh, canned, frozen, or dried-and 100% juice, which are often nutrient-dense forms. Some fruit is consumed through sources that are not nutrient-dense; for example, fruit as part of a baked dessert or juice drink. Beginning at age 9 the amount of dairy foods in a healthy dietary pattern increases from 2 Ѕ to 3 cup equivalents per day to support an increase in calcium intake that is needed during these life stages. As a result, average intake of dairy foods is close to or at recommended levels for children younger than age 9 while consumption among adolescents is typically below recommended intake levels. Although the gaps between recommended and current intakes widen throughout these life stages for some dietary components, others, principally whole grains and seafood, are infrequently consumed by any youth. As the difference between recommended and current intakes widens across age groups, the types of refined and whole-grain foods consumed remains consistent. Mixed dishes, such as pizza, pasta, sandwiches, burgers, and tacos, contribute about 50 percent of total grains intake, and snacks and sweets, such as chips, crackers, and cookies, about 20 percent. Breakfast cereals and bars, including readyto-eat and cooked varieties, are the top contributor to whole-grains intake during these life stages. Despite the underconsumption of whole grains, intakes of total grains trend toward overconsumption due to the contribution of refined grains. Total protein intake generally meets targets except for adolescent females ages 14 through 18. Seafood, a protein subgroup that can support intakes of beneficial fatty acids, is consumed at levels far below the lower end of the recommended intakes range.
Postprandial hyperglycemia in patients with noninsulin-dependent diabetes mellitus: role of hepatic and extrahepatic tissues ulterior motive meaning purchase 12.5mg hydrochlorothiazide amex. Effects of type 2 diabetes on the ability of insulin and glucose to regulate splanchnic and muscle glucose metabolism: evidence for a defect in hepatic glucokinase activity arteria revista hydrochlorothiazide 12.5mg with mastercard. Disordered fat storage and mobilization in the pathogenesis of insulin resistance and type 2 diabetes prehypertension spanish cheap hydrochlorothiazide 25mg with amex. Modulation of hepatic glucose production by non-esterified fatty acids in type 2 (non-insulin-dependent) diabetes mellitus blood pressure 100 over 60 discount 25 mg hydrochlorothiazide otc. Interaction between glucose and free fatty acid metabolism in human skeletal muscle. Effects of free fatty acid availability, glucagon excess, and insulin deficiency on ketone body production in postabsorptive man. Lipolysis during fasting: decreased suppression by insulin and increased stimulation by epinephrine. Effects of exercise and weight loss on leucine turnover in different types of obesity. Turnover and splanchnic metabolism of free fatty acids and ketones in insulindependent diabetics at rest and in response to exercise. Adipose tissue metabolism in obesity: lipase action in vivo before and after a mixed meal. Insulin doseresponse characteristics for suppression of glycerol release and conversion to glucose in humans. Effects of free fatty acids and glycerol on splanchnic glucose metabolism and insulin extraction in nondiabetic humans. Studies in whole body potassium and whole body nitrogen in newly diagnosed diabetics. On diabetic acidosis: a detailed study of electrolyte balances following the withdrawal and reestablishment of insulin therapy. Effect of poor diabetic control and obesity on whole body protein metabolism in man. Protein dynamics in whole body and in splanchnic and leg tissues in type 1 diabetic patients. Effect of exogenous insulin on protein metabolism with differing nonprotein energy intakes in type 2 diabetes mellitus. Effects of oral hypoglycemic agents and diet on protein metabolism in type 2 diabetes. Determinants of whole-body protein metabolism in subjects with and without type 2 diabetes. Cardiovascular risk factors in non-insulin-dependent diabetics compared to nondiabetic controls: a population-based survey among Asians in Singapore. The effect of thiazolidinediones on plasma adiponectin levels in normal, obese, and type 2 diabetic subjects. Failure of suppress plasma glucagon concentrations by orally administered glucose in diabetic patients after treatment. Prevention of human diabetic ketoacidosis by somatostatin: evidence for an essential role of glucagon. Abnormal alpha-cell function in diabetes: response to carbohydrate and protein ingestion. Effect of insulin therapy on the profiles of plasma immunoreactive glucagon in juvenile-type and adult-type diabetics. Perfusion with antiinsulin gamma globulin indicates a B to A to D cellular perfusion sequence in the pancreas of the rhesus monkey, Macaca mulatta. Effect of intermittent endogenous hyperglucagonemia on glucose homeostasis in normal and diabetic man. Effects of long-term optimization and short-term deterioration of glycemic control on glucose counterregulation in type 1 diabetes mellitus.
Describe how you will incorporate the allocation process described in step A in provider order approval blood pressure chart male 25mg hydrochlorothiazide otc. When allocations are utilized prehypertension buy 12.5 mg hydrochlorothiazide overnight delivery, state staff will place orders for all providers receiving vaccine according to allocation plan above arteria femoral buy discount hydrochlorothiazide 12.5 mg line. This tool is based on current functionality for how Michigan currently places public flu prebook orders when allocated doses arterial blood pressure generic hydrochlorothiazide 12.5 mg line. Cold chain must be maintained through the entire transfer, ensuring temperatures are monitored and taken during transport and upon arrival. Pending the format of this submission will dictate any additional technical programming that may be required. At minimum, the Vaccine Primary and Backup Coordinator must fulfill the training requirements. Providers will be educated on taking storage temperatures twice daily, including min/max from digital data loggers. However, we are in discussion in regard to whether providers will also be asked to submit temperature logs for review by the Local Health Department. We are also discussing whether temperatures should be verified prior to approving an enrollment i. Excursion guidance will be provided to ensure providers are aware of how to act on out-of-range temperatures. To do so, we will extract the provider agreement/profile data into an Excel file that generates after completion, allowing us to filter by unit type, number of doses able to store, etc. Ultracold temperature information will be detailed during S&H training and on the website to ensure providers are aware of replenishment expectations as needed. We will work with the Emergency Preparedness team on this to ensure providers have access to dry ice for replenishment as needed. We also discussed the need to instruct on proper handling of dry ice for provider safety. Photos of storage units must also be submitted for approval during the enrollment process. Digital data logger information will be required as well, as continuous monitoring will be necessary. Cold chain must be maintained at all times for satellite, off-site, and temporary vaccination clinics. Planned redistribution from depots to individual locations and from larger to smaller locations i. Redistribution should be limited to refrigerated vaccine and must comply with appropriate storage and handling, ensuring the cold chain is maintained at all times during transport and during receipt at the receiving location. Providers must report to their Local Health Department before redistributing vaccine to ensure appropriate measures will be taken for transport. The state has procured several qualified vaccine transport containers for refrigerated vaccine, as well as digital data logger temperature monitoring devices to support adequate refrigerated transport as needed. Keep in mind ancillary kits when redistributing doses, ensuring the receiving provider receives all necessary components for vaccination. As expected with redistribution and satellite/off-site/temporary clinics, any movement of vaccine must ensure the cold chain is maintained at all times. If unplanned repositioning must occur among provider locations, they must inform the Local Health Department. This will assist in ensuring the reposition is appropriate and that cold chain measures are in place to transfer doses. As discussed above, vaccine storage and temperature monitoring capabilities will be assessed during review enrollment. The storage capabilities will also be used to ensure shipments are directed to providers that can appropriately store and monitor the type of vaccine being ordered for their site. As mentioned above, discussions are ongoing about whether we will request temperature submissions from the provider on a routine basis. Redistribution can only occur in circumstances where the cold chain can be maintained using appropriate transport methods and temperatures monitored throughout. These expectations will be included on the S&H provider website and communicated during the enrollment process. State-procured digital data loggers and transport coolers may be utilized to assist efforts for transferring vaccine if needed. Training will include ensuring providers understanding of how to report vaccinations should systems fail or are temporarily unavailable.
Syndromes
First blood pressure medication starting with n cheap 25 mg hydrochlorothiazide with mastercard, they lacked standardized definitions of depressive disorders pulse pressure 39 buy hydrochlorothiazide 25 mg with visa, mainly using rating scales of unknown reliability and validity in a diabetic population hypertension 8 weeks pregnant order hydrochlorothiazide 25 mg free shipping. The "gold standard" for ascertainment of case status is a research diagnostic interview; most rating scales can only give a probabilistic estimate of caseness arrhythmia in 4 year old order 25mg hydrochlorothiazide amex. In addition, there may be an overlap between symptoms of diabetes and those of depression. Second, studies have tended to ignore the heterogeneity of people with diabetes, studying mixed populations of patients with different forms of diabetes. Third, studies have often been based on "convenience" samples of patients, usually drawn from diabetic clinics, where the operation of referral and other biases in sample composition was of unknown effect. Ethnicity is also an important confounder for rates of both depression and diabetes. Finally, studies have had low or unknown response rates, and because the presence of depressive symptoms may reduce the likelihood of responding in such studies, this biases prevalence estimates further. Not surprisingly, as a result the range of prevalence figures that can be found in the literature is very wide. More recent studies, using better methods, and meta-analyses, have led to lower estimates of prevalence. Caution is still needed in the interpretation of this finding, because it was based on only 14 studies, of which only four included control groups and only seven were based on interview methods. Excluding studies without control groups and interview ascertainment led to a fall in estimated prevalence to 7. This definition is to some degree arbitrary; however, it approximates to a level of symptomatology that is associated with significant disability and dysfunction, and is very widely accepted as a standard in both clinical practice and research. It is important to note that depressive disorders of lesser severity may still compromise self-care and outcomes in people with diabetes. The clinical category of mood disorders includes both unipolar depression and bipolar ("manic-depressive") illness. This section focuses on unipolar depression; bipolar illness is included in the section on psychotic disorders. Five or more of the listed symptoms should be present nearly every day, for at least 2 weeks, and should represent a change from normal functioning; at least one of the first two symptoms in the list must be present Symptoms 1 Depressed mood for most of the day 2 Markedly diminished interest or pleasure in all, or almost all, activities for most of the day 3 Significant weight loss when not dieting, or weight gain (change of 5%), or decrease or increase in appetite 4 Insomnia or hypersomnia 5 Psychomotor agitation or retardation 6 Fatigue or loss of energy 7 Feelings of worthlessness or excessive or inappropriate guilt 8 Diminished ability to think or concentrate 9 Recurrent thoughts of death or suicidal ideation 941 Part 10 Diabetes in Special Groups disease subtype. The effect remained after adjustment for covariates such as cardiovascular disease and obesity. Depressive disorders as a risk factor for diabetes the suggestion that emotional factors, such as grief or sadness, could lead to the onset of diabetes was first raised by Thomas Willis in 1684. A recent systematic review has addressed the question of the direction of the association between these conditions, and summarized the evidence that depression may be a risk factor for diabetes [7]. Unfortunately, the vast majority of existing studies are cross-sectional and therefore uninformative about this issue. Shared genetic risk Another suggested mechanism that may link diabetes and psychiatric disorder is that of shared genetic variance. There is some evidence that close relatives of people with some forms of psychiatric disorder have an increased incidence of diabetes [12], and known loci for the disorders occur in overlapping positions within chromosomes [13]. Investigation of this intriguing possibility is in its infancy and further research is needed. It is thought that such cytokines may be released in increased amounts from adipose tissue in conditions including diabetes and obesity as people age, and this may interfere with insulin action. Loss of normal diurnal variation in cortisol levels together with non-suppression of cortisol release in response to exogenous steroid administration have long been noted as hallmarks of depressive illness, particularly the "melancholic" subtype. It is suggested that this may lead to increased glycogenolysis, gluconeogenesis, lipolysis and inhibition of peripheral glucose transport and utilization [15]. Non-diabetic patients with depression have been shown to have increased insulin resistance, but further investigation of this mechanism is warranted. Glucose transport in the brains of people with depression has also been shown to be abnormal [15]. Proposed mechanisms linking depression and diabetes Psychosocial factors Most studies confirm that risk factors for depression in otherwise healthy individuals operate equally in people with diabetes. Thus, socioeconomic hardship, poor education, stressful life events and lack of social support are all important [8]. There is relatively little evidence that people with diabetes differ greatly with respect to these types of risk factors, and it can be concluded that much depression in people with diabetes may be "independent" of the presence of the disease, an issue that may be particularly important when it comes to management planning.